
ANH in Complex Cardiac Surgery: A Prospective Randomized Study
Abstract
Objectives
Blood transfusions in cardiac surgery are associated with increased morbidity and mortality. The purpose of this study is to identify potential benefits of ANH in high-risk cardiac surgery.
Design
This was a prospective, randomized, controlled study.
Setting
The study was performed at a tertiary care university hospital.
Participants
61 patients who underwent complex cardiac surgery with cardiopulmonary bypass (CPB) were enrolled in the study.
Measurements and Main Results
After randomization, 32 patients were assigned to the ANH arm, and 29 patients were assigned to the control group. ANH was associated with a lower incidence of total perioperative pRBC transfusion (0.6 ± 1.2 units vs 2.7 ± 6.8 units; p = 0.030/0.049). Total perioperative transfusion of all other fractionated blood products, including platelets (0.8 ± units vs 1.9 ± 2.4 units; p=0.010), cryoprecipitate (0.5 ± 0.7 vs 1.3 ± 2.0; p=0.016) and FFP (0.5 ± 1.0 vs 2.3 ± 6.2 units; p=0.013), was significantly lower in the ANH group compared to controls. Participants in the ANH group received significantly fewer intraoperative transfusions of pRBC (0.4 ± 1.2 vs 2.6± 7.0 units; p=0.037), platelets (0.8 ± 1.2 units vs 1.9 ± 2.4 units; p=0.013, logtrans),
FFP (0.4 ± 0.9 vs 2.5 ± 6.4 units; p=0.003) and cryoprecipitate (0.5 ± 0.7 vs 1.3 ± 2.1 units; p=0.012, logtrans). With respect to secondary clinical outcomes, ANH participants had statistically shorter ICU (3.7 ± 1.9 vs 5.4 ± 3.6 days; p=0.020) and hospital (6.7 ± 2.1 vs 9.5 ± 7.7 days; p = 0.048) length of stays
Conclusions
ANH in complex cardiac surgical patients is safe and may be effective in reducing the allogenic blood product transfusion of PRBCs, FFP, platelets and cryoprecipitate in the perioperative period.
Author Contributions
Academic Editor: Anubha Bajaj, Consultant Histopathologist, A.B. Diagnostics, Delhi, India
Checked for plagiarism: Yes
Review by: Single-blind
Copyright © 2025 Lorraine N. Lubin, et al
 This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Competing interests
The authors have declared that no competing interests exist.
Citation:
Introduction
Bleeding in cardiac surgery is a frequent complication. Despite transfusion algorithms and point of care coagulation testing, transfusion of erythrocytes, platelets, and plasma is very common even in low risk cardiac surgery1. Previous studies demonstrate that allogeneic blood transfusions occur in 40-90% of cardiac surgery2.
Packed red blood cells (PRBCs) are associated with worse short-term and long-term outcomes including mortality, renal failure and neurologic complications. Patients who receive a blood transfusion during a cardiac surgical hospitalization have a 70% increase in mortality compared to patients who did not receive a transfusion3.
Acute normovolemic hemodilution (ANH) is a blood conservation technique that may decrease allogeneic blood transfusion in cardiac surgery. Most of the literature for ANH has been studied in low-risk cardiac surgery, such as coronary artery bypass grafting and isolated valve surgery4. There is a paucity of evidence for ANH in high-risk cardiac surgery, such as aortic surgery and adult congenital heart disease surgery. Rates of transfusion in high-risk cardiac surgery are more common than low risk cardiac surgery, therefore, ANH may offer significant potential benefits. However, it is unknown whether ANH is safe and effective in high-risk cardiac surgery. The goal of this study is to assess the effect of ANH on outcomes in patients undergoing high-risk cardiac surgery. We tested the primary hypothesis that ANH reduces perioperative transfusion of erythrocytes within 72 hours following cardiopulmonary bypass. Secondarily, we tested the hypothesis that ANH reduces intraoperative erythrocyte transfusion and erythrocyte transfusion within 24 and 48 hours following cardiopulmonary bypass.
Methods
Study population and design
This study was a single center, prospective, randomized study for adult patients undergoing complex heart surgery as defined by redo sternotomy, aortic surgery, or adult congenital heart disease surgery approved by the IRB. Inclusion criteria included all patients greater than 18 years old presenting for elective cardiac surgery requiring cardiopulmonary bypass. Exclusion criteria included baseline anemia (Hct < 39%/Hgb < 13 g/dL for men and Hct <36%/Hgb < 12 g/dL for women) or a post-dilutional Hct < 21-24 g/dL, heart failure with reduced left ventricular ejection fraction < 35%, acute congestive heart failure, underlying liver disease, chronic kidney disease stage 3 or greater, acute endocarditis, patients on mechanical circulatory support, or emergency cases.
ANH protocol and anesthesia care
Patients presenting for cardiac anesthesia received similar care including an arterial line, a central line introducer and pulmonary artery catheter, transesophageal echocardiography, and cerebral oximetry. Patients were randomized to the ANH or placebo group once the prebypass hematocrit (Hct) value ruled out baseline anemia. The following equations were used to calculate the estimated hematocrit upon initiation of cardiopulmonary bypass (post-dilutional Hct) with and without ANH.
Estimated post-dilutional Hct without ANH = (Hct * Weight * Blood Volume) / ((Blood Volume *Weight) + Bypass Prime volume + crystalloid pre bypass)
Estimated post-dilutional Hct with ANH = ((Hct * Weight * Blood Volume) – (Hct * ANH volume)) /
((Blood Volume *Weight) + Bypass prime volume + crystalloid pre-bypass + ANH volume)
Hematocrit (Hct) is reported as a proportion (0.xx). Weight (Wt) is reported in kilograms. Blood volume (BV) is reported as cc/kg and is estimated using the following weight- based ranges:
85cc/kg (0-10kg), 80cc/kg (11-20kg), 75cc/kg (21-30kg), 70cc/kg (31-40kg) and 65cc/kg (>40kg).
Crystalloid pre-bypass is the volume in (cc) given by anesthesiology providers.prior to bypass, which is typically 400-500 cc. ANH volume (cc) is the volume of whole blood that is removed and replaced with an equivalent volume of crystalloid. The prime volume is 1200cc (small adult CPB circuit) for patients less than 70kg and 1400cc (adult CPB circuit) for patients greater than 70kg. Patients with pre-ANH or post-ANH post- dilutional Hct lower than 22-24% were not eligible for the study.
For the treatment group, ANH was performed by removing 8-10cc/kg of whole blood with a maximum of 700cc from the patient through a 9 French central line
introducer in the operating room prior to incision. Whole blood was collected in standard citrate phosphate dextrose adenine bags (Fresenius Kabi AG Fenwal Blood-Pack Units) and stored at room temperature. Each bag contained 63ml of citrate phosphate dextrose adenine (anticoagulant) solution. After whole blood removal, the patient was hydrated with an equivalent volume of crystalloid and/or colloid given. After cardiopulmonary bypass (CPB) was complete and protamine was given, the whole blood (ANH) was returned to the patient.
For treatment and control groups, we followed the recommendations of the STS/SCA/AmSECT/SABM clinical practice guidelines for patient blood management for all of our patients5. These recommendations included the use of red blood cell salvage using centrifugation, the discontinuation of anti-platelet agents in an appropriate timeframe, the use of synthetic antifibrinolytic agents, retrograde autologous priming, the use of a restrictive perioperative allogeneic RBC transfusion strategy, and a goal directed transfusion algorithm which incorporated point of care testing.
The following transfusion algorithm was used 6, 7 :
ACT > 130 seconds -> Protamine 30 units/kg
PRBC administered for a Hemoglobin < 7 g/dL
Platelets administered for a platelet count < 80,000 /uL with surgical bleeding
Fresh frozen plasma administered for an CT Ex > 80 seconds or CT Hep > 240 seconds
Cryoprecipitate administered for a A10Fib < 10mm and A10Ex < 40mm
Statistical Analysis
Patient characteristics, intraoperative variables, laboratory results, and clinical outcomes were summarized overall in Table 1, Table 2, Table 3 and by study group (ANH vs control) using means and standard deviations for continuous variables and frequencies with percentages for categorical variables. Comparisons between groups were conducted using independent-sample t-tests for continuous variables and chi-square tests for categorical variables. For transfusion-related outcomes (e.g., perioperative and intraoperative pRBCs, platelets, FFP, cryoprecipitate), which exhibited skewed distributions, log transformation was applied prior to conducting group comparisons with t-tests. Additional comparisons for secondary outcomes, such as ICU and hospital length of stay, were also assessed using t-tests. All analyses were conducted using SPSS version 28 (IBM Corp., Armonk, NY) and R version 4.1.0 (R Foundation for Statistical Computing, Vienna, Austria). All tests were two-tailed, and p-values < 0.05 were considered statistically significant.
Power and sample size
The planned sample size was based on detecting a reduction in the proportion of patients receiving perioperative pRBC transfusion from 60% to 30%, requiring 112 patients with 80% power at a two-sided alpha of 0.05. However, the study was terminated early after enrollment of 61 patients due to staffing and resource limitations.
Results
Sixty-one patients that met both inclusion and exclusion criteria were enrolled in the study between February 2022 and May 2023. After randomization, 32 patients (52%) were assigned to the ANH arm while the remaining 29 patients were assigned to the control group. Participant demographics and perioperative features are shown in Table 1
Table 1. Demographics| Overall (N=61) | Control (N=29) | ANH (N=32) | p-value | |
| Demographics | ||||
| Age (years) | 55.3 (17.4) | 60.3 (14.8) | 50.9 (18.6) | 0.034 |
| Female gender | 17 (27.9%) | 9 (31.0%) | 8 (25.0%) | 0.6 |
| Weight (kg) | 84.6 (20.7) | 85.7 (21.6) | 83.6 (20.1) | 0.694 |
| Height (cm) | 173.6 (11.9) | 170.9 (14.0) | 176.0 (9.1) | 0.094 |
| Preoperative Cardiac Function | ||||
|---|---|---|---|---|
| LVEF (%) | 58.5 (9.1) | 57.2 (9.3) | 59.7 (9.0) | 0.291 |
| NYHA class | 0.27 | |||
| 1 | 5 (8.2%) | 4 (13.8%) | 1 (3.1%) | |
| 2 | 37 (60.7%) | 17 (58.6%) | 20 (62.5%) | |
| 3 | 18 (29.5%) | 7 (24.1%) | 11 (34.4%) | |
| 4 | 1 (1.6%) | 1 (3.4%) | 0 (0%) | |
| Preoperative Liver Function | ||||
| AST (U/L) | 27.9 (15.1) | 31.0 (20.0) | 24.7 (6.4) | 0.11 |
| ALT (U/L) | 27.2 (18.9) | 30.8 (22.9) | 23.5 (13.2) | 0.14 |
| Preoperative Renal Function | ||||
| Creatinine (mg/dL) | 1.0 (0.2) | 1.0 (0.2) | 1.0 (0.3) | 0.831 |
| Preoperative Hematologic Studies | ||||
| Hgb (g/dL) | 13.6 (1.6) | 13.5 (1.7) | 13.6 (1.5) | 0.815 |
| Platelet (x 10E 3/uL) | 211.8 (55.9) | 197.4 (61.8) | 224.9 (47.1) | 0.054 |
| Preoperative Coagulation Studies | ||||
| INR | 1.1 (0.1) | 1.1 (0.1) | 1.1 (0.2) | 0.424 |
| PTT (sec) | 31.6 (11.1) | 33.6 (15.6) | 30.0 (5.0) | 0.256 |
| Fibrinogen (mg/dL) | 228.6 (75.2) | 247.2 (80.4) | 203.8 (63.5) | 0.197 |
| Antiplatelet agents | 2 (3.3%) | 0 (0%) | 2 (6.2%) | 0.493 |
| LMWH agents | 0 (0%) | 0 (0%) | 0 (0%) | 1 |
| Surgical considerations | ||||
| Surgical procedures | 0.433 | |||
| Complex aortic surgery | 35 (57.4%) | 18 (62.1%) | 17 (53.1%) | |
| Complex ACHD | 18 (29.5%) | 6 (20.7%) | 12 (37.5%) | |
| Complex valve with concomitant procedure | 6 (9.8%) | 4 (13.8%) | 2 (6.2%) | |
| Myomectomy and valve repair | 2 (3.3%) | 1 (3.4%) | 1 (3.1%) | |
| Repeat sternotomy | 18 (29.5%) | 10 (34.5%) | 8 (25.0%) | 0.417 |
Baseline characteristics between the ANH and control groups were comparable except that participants in the ANH group were found to be younger (50.9 ± 18.6 vs 60.3 ± 14.8; p = 0.034). The preoperative hematologic and coagulation profiles between both groups were similar. Furthermore, no differences between groups were noted in the estimated/calculated and actual post-dilutional hematocrit.
Intraoperative characteristics are presented in Table 2. As demonstrated in Table 2, no statistical differences in CPB time, aortic cross-clamp time, circulatory arrest time, or number of pump runs were observed between groups. The lowest recorded temperature on CPB was statistically higher in the ANH group compared to controls (32.1 ± 4.3 °C vs 29.6 ± 5.4 °C; p=0.050). Intraoperative administration of crystalloid and colloid as well as heparin and protamine were similar between both groups. There was comparable utilization of antifibrinolytics (aminocaproic acid or tranexamic acid), desmopressin, prothrombin complex concentrate and recombinant factor VIIa in both groups. Utilization of inotropic support was the same between both groups. No intragroup difference was observed in the incidence and medical management of vasoplegia.
Table 2. Intraoperative| Overall (N=61) | Control (N=29) | ANH (N=32) | p-value | |
| Cardiopulmonary bypass | ||||
| CPB time (min) | 189.4 (98.7) | 208.4 (105.7) | 172.1 (90.2) | 0.154 |
| Aortic cross clamp time (min) | 135.7 (75.9) | 141.4 (70.5) | 130.3 (81.4) | 0.576 |
| Circulatory arrest | 9 (14.8%) | 7 (24.1%) | 2 (6.2%) | 0.072 |
| Circulatory arrest (min) | 26.7 (27.1) | 29.4 (30.6) | 17.0 (4.2) | 0.602 |
| Multiple pump runs | 8 (13.1%) | 3 (10.3%) | 5 (15.6%) | 0.71 |
| Pump runs (count). | 2.6 (0.9) | 2.7 (1.2) | 2.6 (0.9) | 0.929 |
| Heparin (10e3 units) | 30.6 (7.5) | 31.8 (7.3) | 29.4 (7.7) | 0.224 |
| Protamine (mg) | 235.7 (75.4) | 238.6 (93.8) | 233.0 (55.3) | 0.774 |
| ANH characteristics | ||||
| Estimated pre-ANH post- dilutional Hct | 31.5 (3.6) | 31.1 (4.0) | 31.9 (3.2) | 0.441 |
| Estimated post-ANH post-dilutional Hct | 26.1 (3.2) | 26.2 (3.7) | 26.0 (2.8) | 0.78 |
| Estimated ANH Volume | 342.6 (325.3) | 20.7 (111.4) | 634.4 (93.7) | <0.001 |
| Blood transfusions | ||||
| pRBC (units) | 1.4 (4.9) | 2.6 (7.0) | 0.4 (1.2) | |
| FFP (units) | 1.4 (4.5) | 2.5 (6.4) | 0.4 (0.9) | |
| Platelet (units) | 1.3 (1.9) | 1.9 (2.4) | 0.8 (1.2) | |
| Cryo (units) | 0.9 (1.5) | 1.3 (2.1) | 0.5 (0.7) | |
| Procoagulant factors/Hemostatic agents | ||||
| Factor VIIa | 2 (3.3%) | 2 (6.9%) | 0 (0%) | |
| PCC | 4 (6.6%) | 3 (10.3%) | 1 (3.1%) | 0.338 |
For the primary outcome, there was no statistical difference in total postoperative pRBC transfusions between the ANH and control group (0.2 ± 0.5 units vs 0.3 ± 0.6 units; p = 0.402) as shown in Table 3. Receipt of ANH was associated with a lower incidence of total perioperative pRBC transfusion (0.6 ± 1.2 units vs 2.7 ± 6.8 units; p = 0.030/0.049). Total perioperative transfusion of all other fractionated blood products, including platelets (0.8 ± units vs 1.9 ± 2.4 units; p=0.010), cryoprecipitate (0.5 ± 0.7 vs 1.3 ± 2.0; p=0.016) and FFP (0.5 ± 1.0 vs 2.3 ± 6.2 units; p=0.013), was significantly lower in the ANH group compared to controls. Participants in the ANH group received significantly fewer intraoperative transfusions of pRBC (0.4 ± 1.2 vs 2.6 ± 7.0 units; p=0.037), platelets (0.8 ± 1.2 units vs 1.9 ± 2.4 units; p=0.0.13, logtrans), FFP (0.4 ± 0.9 vs 2.5 ± 6.4 units; p=0.003) and cryoprecipitate (0.5 ± 0.7 vs 1.3 ± 2.1 units; p=0.012, logtrans). Postoperative transfusions of pRBCs, platelets, FFP and cryoprecipitate at 24, 48 and 72 hours did not differ between ANH and control groups.
With respect to secondary clinical outcomes, ANH participants had statistically shorter ICU (3.7 ± 1.9 vs 5.4 ± 3.6 days; p=0.020) and hospital (6.7 ± 2.1 vs 9.5 ± 7.7 days; p = 0.048) length of stays (Table 5). There were no statistically significant differences in postoperative intubation time, left ventricular systolic function, and re-exploration for bleeding. The incidence of neurologic complications including stroke and renal failure requiring dialysis were the same between groups. Perioperative myocardial injury/infarction and death occurred a similar frequency in the ANH and control groups.
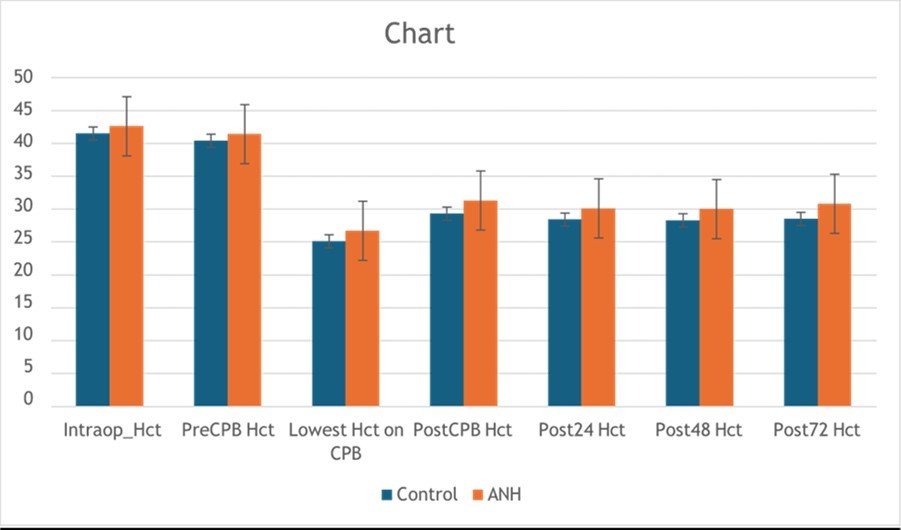
Table 3. Post-ANH Laboratory Studies| Overall (N=61) | Control (N=29) | ANH (N=32) | p-value | |
| Hct | ||||
| Post-OR | 30.4 (5.3) | 29.3 (6.1) | 31.3 (4.3) | 0.141 |
| 24hr Post-OR | 29.3 (5.3) | 28.4 (5.0) | 30.1 (5.5) | 0.22 |
| 48hr Post-OR | 29.2 (5.3) | 28.3 (4.6) | 30.0 (5.9) | 0.218 |
| 72hr Post-OR | 29.7 (5.4) | 28.5 (4.6) | 30.8 (5.8) | 0.095 |
| Platelet count () | ||||
| Post-OR | 144.3 (47.3) | 151.9 (52.3) | 137.1 (41.8) | 0.229 |
| 24hr Post-OR | 127.3 (42.5) | 139.4 (48.8) | 116.1 (32.6) | 0.032 |
| 48hr Post-OR | 128.1 (45.2) | 127.5 (42.8) | 128.6 (47.8) | 0.928 |
| 72hr Post-OR | 161.9 (69.2) | 158.0 (57.3) | 165.3 (78.9) | 0.684 |
| INR | ||||
| Post-OR | 1.4 (0.2) | 1.4 (0.3) | 1.3 (0.2) | 0.353 |
| 24hr Post-OR | 1.3 (0.2) | 1.3 (0.2) | 1.4 (0.2) | 0.109 |
| 48hr Post-OR | 1.3 (0.3) | 1.3 (0.2) | 1.4 (0.3) | 0.831 |
| 72hr Post-OR | 1.5 (0.5) | 1.6 (0.5) | 1.4 (0.3) | 0.71 |
| PTT (sec) | ||||
| Post-OR | 35.0 (8.5) | 36.5 (10.0) | 33.6 (6.6) | 0.308 |
| 24hr Post-OR | 35.8 (12.8) | 34.5 (6.1) | 37.3 (17.8) | 0.55 |
| 48hr Post-OR | 46.4 (50.4) | 54.9 (69.8) | 37.0 (7.5) | 0.457 |
| 72hr Post-OR | 39.8 (20.2) | 37.8 (10.5) | 41.6 (26.7) | 0.71 |
| Fibrinogen (mg/dL) | ||||
| Post-OR | 201.3 (42.6) | 207.0 (39.3) | 196.3 (45.6) | 0.396 |
| 24hr Post-OR | 208.0 (50.9) | 215.2 (64.3) | 196.0 (20.7) | 0.643 |
| 48hr Post-OR | ||||
| 72hr Post-OR | ||||
| Creatinine (mg/dL) | ||||
| Post-OR | 1.0 (0.3) | 1.0 (0.3) | 1.0 (0.3) | 0.919 |
| 24hr Post-OR | 1.0 (0.6) | 1.0 (0.4) | 1.0 (0.7) | 0.929 |
| 48hr Post-OR | 1.1 (0.6) | 1.1 (0.4) | 1.0 (0.7) | 0.708 |
| 72hr Post-OR | 1.0 (0.6) | 1.0 (0.4) | 1.0 (0.6) | 0.758 |
| Lactate (mg/dL) | ||||
| Post-OR | 27.2 (22.7) | 29.1 (24.1) | 25.4 (21.6) | 0.565 |
| 24hr Post-OR | 16.3 (9.5) | 19.3 (12.2) | 14.1 (6.7) | 0.15 |
| 48hr Post-OR | 13.6 (6.0) | 12.3 (4.1) | 14.7 (7.3) | 0.403 |
| 72hr Post-OR | 11.1 (5.2) | 9.8 (6.0) | 11.8 (5.0) | 0.554 |
Discussion
Our study ANH in Complex Cardiac Surgery is a prospective, randomized, controlled study conducted at a large academic university hospital. We embarked on this study with the idea that ANH has been shown to be a safe and efficacious blood conservation strategy in low-risk cardiac surgery and has been shown to diminish red blood cell transfusion8. There have been no known prospective, randomized trials looking at ANH in complex cardiac surgery. The patients included in the study had complex valve, aortic, valve-CABG, redo sternotomy and adult congenital heart open-heart procedures requiring cardiopulmonary bypass. Our study excluded any single valve procedures, CABG surgery, heart transplants and patients with acute heart failure, left ventricular ejection fraction lower than 35%, anemia, recent transfusion, infection, malignancy, and dialysis dependent renal failure. All patients had ROTEM and laboratory driven standardized transfusion guidelines in the perioperative period, and there were no complications experienced in the study. There was a single neurological death in the control group.
The primary outcome of decreased PRBC transfusion in the perioperative period was statistically significant over the cumulative 72-hour perioperative interval. The intraoperative period had similar PRBC transfusion rates in both the study and control groups. We attributed this finding to the case selection. Both the control and ANH groups incurred heavy bleeding and required red blood cell transfusion which remained necessary and similar in both groups during that immediate, operative period. However, when we evaluated the total PRBC transfusion over the 72-hour perioperative interval, we found the difference in total red cell transfusion between the ANH and control groups to be different with the ANH group requiring significantly diminished red cell transfusion requirements. These findings have important clinical and economic implications. Transfusions of all blood products are known to be resource and cost- intensive and have been shown to increase perioperative complications, morbidity and mortality. In cardiac surgery, pulmonary and cardiac dysfunction, neurologic impairment, infection and renal failure are major concerns and have been increased in patients receiving transfusions9. Therefore, incorporating a blood conservation strategy like ANH which may reduce transfusion requirements and diminish exposure to blood products may reduce morbidity, mortality and costs.
Important statistically significant secondary outcomes including diminished transfusion of platelets, cryoprecipitate, FFP, total blood product transfusion, decreased length of intensive care unit stay and decreased length of hospital stay were seen in the ANH group. The clinical impact of reduced transfusion on complex cardiac surgical patients is most likely multifactorial. Kotake et. al. found a difference in autologous blood transfusion-induced inflammatory responses between ANH and preoperatively donated autologous blood. The Kotake group reported that ANH blood transfusions were associated with a smaller concentration of inflammatory mediators such as interleukin 10 and neutrophil elastase than autologous blood bank blood10. Liker et al. previously described the cardioprotective effects of ANH in patients undergoing coronary artery bypass surgery due to the hemodilution-induced blood viscosity. Cardio-protection may be associated with improved oxygen supply and consumption balance11. A reduction in postoperative pulmonary infections has previously been described, although no difference in ventilator days was seen in the study by Zhou et al12. as well as our group. Our study had a limit of 700 cc of ANH blood removal. There was a greater benefit with a larger volume of ANH blood removed. The most common amount removed was 600 cc due to the collection bag size and ratio of preservation fluid (citrate phosphate dextrose adenine). The average volume removed was 652 cc. 8-10 cc/kg was the recommended removal volume. However, there were ten patients who received 700- 1000 cc of ANH. In these patients, whole blood removed and reinfused was well tolerated. A single ACHD patient weighing 133 kg had 1000 cc removed due to high hematocrit (48%) and good hemodynamics per the care team. This practice was consistent with the report of Goldberg et al13. and the meta-analysis by Barile et al8.
Both studies reported a reduction in PRBC transfusion by using an ANH blood conservation technique and described a dose-dependent response in which patients receiving larger volume ANH had diminished blood bank blood requirements. It is possible that previous studies using small and medium volume ANH failed to show benefit due to the reduced ANH volume13.
The use of cell saver blood scavenging technique, antifibrinolytic medication with tranexamic acid and aminocaproic acid along with ROTEM evaluation likely augmented our ANH blood conservation and may be considered standard practice in cardiac surgery. However, it is unknown to what extent these practices may have impacted our study. We used these techniques on all patients enrolled in the study.
A trend toward the early use of recombinant coagulation factors such as Factor VII concentrate, Prothrombin complex concentrate (PCC, Kcentra) and Factor IX complex (Profiline) is evolving in cardiac surgical practice14. In our study, PCC was used as a rescue technique after it was determined the coagulopathy was severe and required recombinant factors based on ROTEM and minimal response to transfused blood products. We had four patients who required the use of PCC. Two of the patients were adult congenital heart disease cases with complex repairs with redo sternotomies who required circulatory arrest. One of the ACHD patients was a control and the other received ANH. The other two patients were complex, double valve, hemiarch cases and both were randomized to the control arm. Three of these patients required hypothermia to below 24 degrees or circulatory arrest and the fourth case experienced an aortic cross clamp time of 150 min at 32 degrees. In these cases, it is thought that profound hypothermia and prolonged cardiopulmonary bypass contributed to the significant, refractory coagulopathy.
The human factor of the ANH technique and process should be appreciated. The process adds another level of complexity to an already complicated procedure. The technique requires vigilance in removing a large amount of blood volume from a hemodynamically fragile patient in a sterile fashion with the appropriate amount of anticoagulant. The blood must be oscillated to prevent clot formation and reinfused within an 8-hour period. However, the benefits of the technique are that the autologous whole blood once collected serves as an in operating room “blood bank” for the patients to receive undiluted, fresh whole blood which contains red cells and critical coagulation factors in a proportionally appropriate amount without the risks of foreign blood product exposure. In our study, there were no clot formations reported. No wastage of ANH blood units occurred, and no complications were reported with respect to collection or reinfusion. All patients had a rigorous screening process which calculated the pre- and post-dilutional hematocrits that would have been anticipated after the ANH removal and the dilutional hematocrit anticipated on cardiopulmonary bypass. Patients with a dilutional hematocrit lower than 22% were excluded from the study. There was no difference in lactate levels, incidence of AKI, decreased brain saturation, hemodynamic instability, incidence of cardiac ischemia or other complications in either the ANH or control groups. This screening process was an additional level of safety that helped us select appropriate patients for the study. Patient selection for the ANH technique is vital as well as meticulous technique to avoid hemodynamic compromise. Attention to positioning in Trendelenburg during collection and gentle fluid administration during removal of blood and replacement cannot be overlooked. With appropriate patient selection and meticulous technique, the safety of ANH was confirmed in our prospective, randomized study.
Limitations
The primary limitations of our study include the unblinded nature of the study due to the technique required, small sample size secondary to the single study site and rigorous patient screening process, and early termination of the study. There was a possible effect of individual physician practice as well as the effect of having the ready, in-place ANH autologous blood units available and ready to give during the immediate post- bypass period, which is frequently characterized by vasoplegia and hypovolemia. All our participating physicians mentioned the convenience of having immediate volume and whole blood ready to infuse as a benefit of the technique when treating complex cardiac surgical patients. This also may have influenced the surgical team from requesting further blood products thus impacting the total products transfused. This may have contributed to a possible performance bias.
Conclusion
This single center, prospective randomized controlled study demonstrated ANH in complex cardiac surgical patients to be safe and effective in reducing the allogenic blood product transfusion of PRBCs, FFP, platelets and cryoprecipitate in the perioperative period. While the efficacy of ANH has been shown in previous studies, there has not been a prospective trial evaluating the technique in complex cardiac surgical cases. While additional studies are needed to identify subgroups which may benefit more from the technique of ANH and the optimal volume; the technique of using ANH as part of a blood conservation strategy is safe and may diminish exposure to blood products as well as show positive outcomes such as decreased ICU and hospital length of stay.
References
- 1.Bennnett-Guerrero E, Zhao Y, O’Brien S M, Ferguson TB Jr, Peterson E D et al. (2010) Song HK: Variation in use of blood transfusion in coronary artery bypass graft surgery. JAMA. 304-1568.
- 2.Stover E P, Siegel L C, Parks R. (1998) Institutions of the Multicenter Study of Perioperative Ischemia Research Group. Variability in transfusion practice for coronary artery bypass surgery persists despite national consensus guidelines: a 24-institution study. Anesthesiology. 88(2), 327-333.
- 3.Engoren M, Habib R, Zacharias A. (2002) Effect of blood transfusion on long term survival after cardiac operation. Ann Thorac Surg. 74(4), 1180-6.
- 4.Spahn D R, Schmid E R, Seifert B, Pasch T. (1996) Hemodilution tolerance in patients with coronary artery disease who are receiving chronic beta-adrenergic blocker therapy. Anesth Analg. 82, 687-694.
- 5.Tibi P, McClure R S, Huang J. (2021) STS/SCA/AmSECT/SABM update to the Clinical Practice Guidelines on Patient Blood Management. , J Extra Corpor Technol 53(2), 97-124.
- 6.Weber C, Meininger D, Herrmann E. (2012) Point of Care Testing: A Prospective randomized Clinical Trial of Efficacy in Coagulopathic Cardiac Surgery Patients. Anesthesiology. 117-531.
- 7.Mazer C, Whitlock R, Fergusson D. (2017) Restrictive or Liberal Red Cell Transfusion for Cardiac Surgery. , NEJM 377-2133.
- 8.Barile L, Fominskly E, Tomasso Di. (2017) Acute Normovolemic Hemodilution Reduces Allogeneic Red Blood Cell Transfusion in Cardiac Surgery: A Systematic Review and Meta-analysis of Randomized Trials. , Anesthesiology 124(3), 743-752.
- 9.Engoren M, Habib R, Zacharias A. (2002) Effect of blood transfusion on long term survival after cardiac operation. Ann Thorac Surg. 74(4), 1180-6.
- 10.Kotake Y, Yamamoto M, Matsumoto M. (2009) . Difference in Autologous blood transfusion-induced Inflammatory Responses Between Acute Normovolemic Hemodilution and Preoperative 23, 61-66.
- 11.Liker M, Ellenberger C, Sierra J. (2005) Cardioprotective Effects of Acute Normovolemic Hemodilution in Patients Undergoing Coronary Artery Bypass Surgery. Chest. 128-838.
- 12.Zhou Z, Jia X, Sun K. (2017) Mild Volume Acute Normovolemic Hemodilution is Associated with Lower Intraoperative Transfusion and Post-Operative Pulmonary Infection in Patients Undergoing Cardiac Surgery- A Retrospective, Propensity Matching Study. , BMC Anesthesiology 17, 1-9.