
Pericardiocentesis Procedure: Anatomical Structures and Approaches
Abstract
Knowledge of accurate surface anatomy is essential for safe clinical practice. Different views and opinions for clinically important surface markings exist between clinicians. Pericardiocentesis is performed as an emergency procedure in conditions aggravating cardiac tamponade. The approach of pericardiocentesis should be held by the hands of an experienced operator because of the surrounding relations. Nowadays, the introduction of imaging-guided procedures, especially echo-guided procedures, has significantly improved the safety and feasibility of pericardiocentesis and has provided the possibility of choosing the best anatomical approach among the apical, subcostal and parasternal approaches. This case report also emphasizes the importance of instillation of agitated saline as a supplementary technique while performing echo-guided pericardiocentesis in order to reduce the likelihood of cardiac chamber perforations.
Author Contributions
Academic Editor: Abdelmonem Awad Mustafa Hegazy, Professor and Former Chairman of Anatomy and Embryology Department, Faculty of Medicine, Zagazig University, Egypt.
Checked for plagiarism: Yes
Review by: Single-blind
Copyright © 2021 Divia Paul Aricatt
 This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Competing interests
The authors have declared that no competing interests exist.
Citation:
Introduction
Pericardiocentesis is the most useful therapeutic procedure for the early management or diagnosis of large, symptomatic pericardial effusion and cardiac tamponade 1. The first description of cardiac decompression was in 1653, when Riolanus suggested sternal trephination to relieve pericardial pressure. In 1911, Marfan first described the subxiphoid approach, which had been used for the blind pericardiocentesis procedure for decades, despite the significant morbidity and mortality rates (50% and 6%, respectively) 2. In the subsequent years, the techniques recommended for a safe and successful pericardiocentesis have changed considerably, particularly with the introduction of fluoroscopic, electrocardiographic and, finally, echocardiographic guidance 3, and with the description of approaches other than the substernal one (apical and parasternal). Pericardiocentesis is performed as an emergency procedure in conditions aggravating cardiac tamponade, or as a part of the diagnostic workup of cryptogenic pericardial effusion 1.Accurate surface anatomy is essential for safe clinical practice. Different views and opinions for clinically important surfacemarkings exist between clinicians. Percutaneous pericardiocentesis was first performed in 1840 by Frank Schuh 2. The subxiphoid approach was adopted in 1911 but because the procedure was performed ‘blind’, it was associated with high rates of complication3. Advanced fluoroscopicand ultrasonic techniques, helped to reduce the complication rates associated with pericardiocentesis between 0.5 and 3.7% 4, 5, 6. Echocardiography has been given class l recommendation by a 2003 task force of the American Heart Association (AHA), and the American Society of Echocardiography (ASE) 7. Echocardiographic diagnosis of pericardial effusion confirms the clinical diagnosis of acute pericarditis. This should be performed prior to performing a pericardiocentesis to document the location and the size of the effusion. Echocardiography can detect an effusion as small as 30 cc 8.
The indications and contraindications of the procedure among haemodynamically unstable patients, pericardiocentesis is an emergent procedure because only the removal of fluid allows a normal ventricular filling and can restore an adequate cardiac output 9, 10. In cases other than emergency, the procedure can be performed within the hours following presentation and the most appropriate visual guidance and approach can be planned. A scoring index has recently been proposed in patients with a suspicion of tamponade for deciding whether to perform urgent pericardiocentesis or drainage later in the subsequent hours. Aetiology, clinical presentation, and echocardiographic findings are the three components which when obtained at initial presentation decide the need of the urgent procedure 11.
In case of pericardial effusion without haemo dynamic compromise, pericardiocentesis is indicated for symptomatic moderate to large effusion non-responsive to medical therapy or, in case of a smaller effusion, when tuberculous, bacterial or neoplastic pericarditis is suspected, or in case of chronic and large pericardial effusion (>20 mm on echocardiography in diastole) 9. Pericardiocentesis for diagnostic purposes is not justified in cases of mild or moderate effusions (<20 mm) for the following reasons: 1) low diagnostic power 2) self-limiting viral (idiopathic) pericarditis which only requires an anti-inflammatory treatment, and 3) high procedural risk compared with low diagnostic yield 12.
There are no absolute contraindications to pericardiocentesis when cardiac tamponade and shock occur. Aortic dissection and post-infarction rupture of the free wall are contraindications to needle pericardiocentesis due to the potential risk of aggravating the dissection or myocardial rupture via rapid pericardial decompression and restoration of systemic arterial pressure. 13. Relative contraindications include uncorrected coagulopathy, anticoagulant therapy, thrombocytopaenia (PLTc<50,000/mm3).
Case Report
We describe a case in which an easy action, such as instillation of agitated saline, allowed us to confirm a major complication related to pericardiocentesis. A 62-year-old man with a history of mitral and aortic valve replacement 2 weeks earlier presented with complaints of dyspnea and asthenia. Laboratory tests and chest x-ray revealed the presence of massive right hemothorax and severe secondary anaemia. Despite blood transfusion and chest tube insertion, the patient’s hemodynamic situation continually worsened, and he finally developed cardiac arrest. During cardiopulmonary resuscitation, an urgent echocardiogram showed severe pericardial effusion. Therefore, pericardiocentesis by a subxiphoid approach was performed. After stabilisation, the patient was transferred immediately to coronary care unit. The pericardial tube had been left in place. Continuous blood drainage was noticed after shifting and agitated saline was injected through the drainage tube to define its precise location. Right ventricular opacification was observed during a repeat echocardiogram with massive bubbles confirming the drainage tube was placed actually within the right ventricle (Figure 1). This case emphasizes the importance of instillation of agitated saline as a supplementary technique while performing echo-guided pericardiocentesis in order to reduce the likelihood of cardiac chamber perforations. Subsequent sections will discuss more frequent complications of pericardiocentesis including rates, severity, and other important procedural and non-procedural considerations.
Figure 1.The complete opacification of the right ventricle (yellow arrow) and the presence of some bubbles within the right atrium (red arrow),denoting that the tip of the drainage tube is malpositioned within the right ventricle.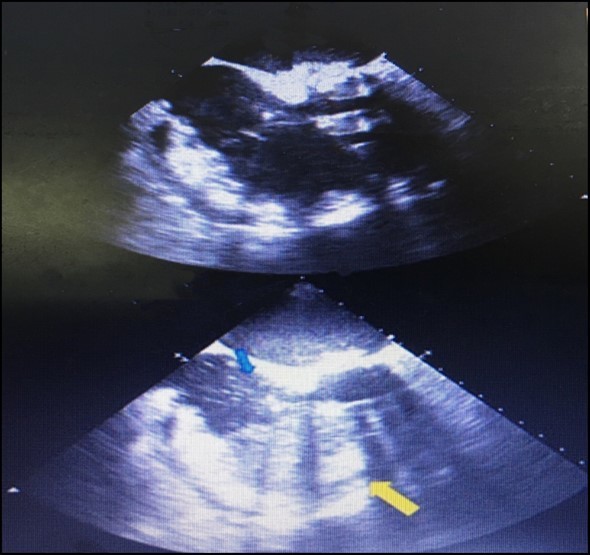
Discussion
Pericardiocentesis: Anatomic structures and approaches are as follows, the pericardium is composed of visceral and parietal components. The pericardial space is enclosed between these two serosal layers and normally contains up to 50 mL of plasma ultra-filtrate, the pericardial fluid 8. The approach of pericardiocentesis should be held by the hands of an experienced operator because of the surrounding relations (Figure 2). Anteriorly, the fibrous pericardium is separated from the thoracic wall by the lungs and the pleural coverings. The direct contact of the pericardium with the thoracic wall is observed in a small area behind the lower left half of the body of the sternum and the sternal ends of left fourth and fifth costal cartilages.
Figure 2.Anatomic structures to be taken care during pericardiocentesis procedure.
The principal bronchi, oesophagus, oesophageal plexus, descending thoracic aorta and posterior parts of the mediastinal surface of both lungs are posterior relations. Laterally, the pleural coverings of the mediastinal surface of the lungs 14. The most commonly employed approach to closed pericardiocentesis is subxiphoid needle insertion 8 in the left fifth or sixth intercostals space near the sternum 14 directed towards the right shoulder. Approach should be done with echocardiographic guidance to minimize the risk of myocardial puncture and to assess completeness of fluid removal 15. Once the needle has entered the pericardial space, a modest amount of fluid should be immediately removed (perhaps 50 to 150 mL) in an effort to produce immediate hemodynamic improvement. A guidewireis then inserted and the needle replaced with a pigtail catheter under echocardiographic guidance to maximum fluid removal 8. ‘The bare area’ of the pericardium formed by the cardiac notch of the left lung and the shallow notch in the left pleural sac makes an easy approach to the pericardial sac. The pericardial sac can be approached through the infrasternal angle i.e; the left costo-xiphoid angle by passing the needle superoposteriorly or up and backwards in to the pericardial sac 16 at an angle of 45 degrees to the skin 17. At this site, the needle avoids the lung and pleurae and enters the pericardial cavity however; care must be taken not to puncture the internal thoracic artery. One of the more difficult management decisions is whether to perform closed verses open pericardiocentesis in patients with known or suspected bleeding in to the pericardial space. In minimised 16. [Figure 3A & B]
Figure 3.A. Anatomic structures to be taken care during pericardiocentesis procedure. B. Three main approaches for pericardiocentesis; a) Parasternal, b) Apical and c) Substernal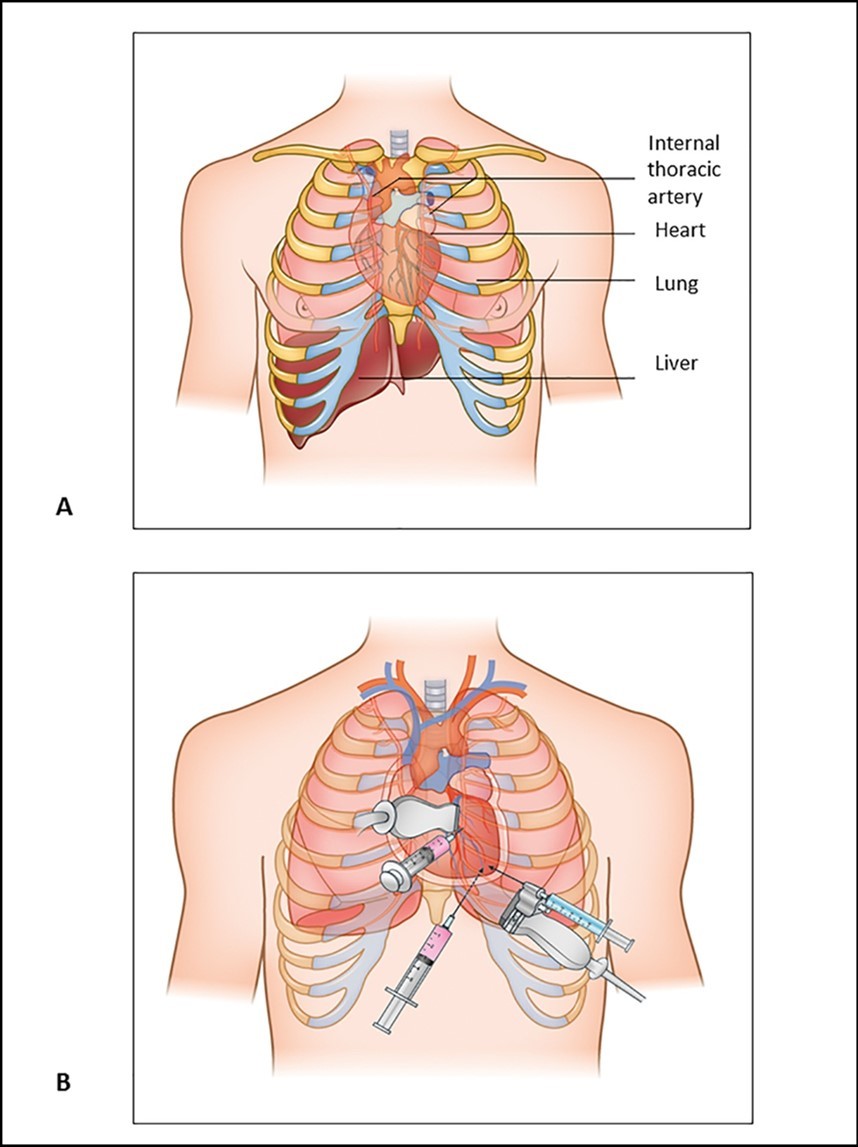
When the procedure is performed, the pleura and lung are not injured because of the presence of the cardiac notch in this area 16. The phrenic nerve, with its accompanying vessels, descends between the fibrous pericardium and mediastinal pleura on each side. Inferiorly, the pericardium is separated by the diaphragm from the liver and fundus of the stomach 14 (Figure 1).Ribs and their counting is done from the second costal cartilage is identified first at the level of sterna angle; thereafter the ribs are palpated and counted downwards and laterally away from the sternum in order to avoid confusion due to crowding of the cartilages of fifth, sixth and seventh ribs as they approach the sternum. The sterna end of the first rib can be felt immediately below the sternal end of the clavicle.
Infra-sternal angle (Subcostal Angle) is at the two subcostal margins enclose or meets ups in the infra-sternal angle. The xiphoid process lies in the shallow depression of infra-sternal angle. The xiphisternal joint is represented by a transverse ridge at the apex of the infrasternal angle.Costal margin is formed by the union of the upturned ends of the cartilages of tenth, ninth, eighth and seventh ribs. The costal margin is usually visible through the skin. Lateral margins of the sternum can be felt indistinctly at the sternal ends of the second,third and fourth intercostals spaces 14.Following pericardiocentesis, repeated echocardiography and continued hemodynamic monitoring are useful to assess reaccumulation. The duration of monitoring is amatter of judgement but typically 24 hours is sufficient 8.Echocardiography-guided pericardiocentesis is a safe and simple technique, introduced at the Mayo Clinic in 1979 and widely used nowadays 18.
The echocardiography-guided approach allows defining the position of the effusion, the ideal entry site and needle trajectory for pericardiocentesis. There are two different approaches to echo guidance: the first is the echo-assisted method, in which the operator memorises the optimal needle trajectory and advances the needle towards the pericardial space without a continuous ultrasound visualisation. The second approach is the echo-guided method with a continuous echocardiographic monitoring. It has also been proposed to use a needle carrier mounted on the ultrasound transducer to advance the needle to the pericardial space 18, 19.
Conclusion
Pericardiocentesis can be a potentially life-saving procedure that carries a high risk of complications. In this regard, imaging support and the careful planning of the proper entry site are fundamental for a safe and successful procedure. The knowledge of surface anatomy will help to render a clear pathway leaving back the darkness of ignorance to perform the procedure ‘Pericardiocentesis’.
References
- 3.Bishop L H, Estes E H, McIntosh H D. (1956) The electro cardiogram as a safeguard in pericardiocentesis. , JAMA 162, 264.
- 4.Duvernoy O, Borowiec J, Helmius G, Erikson U. (1992) Complications of percutaneous pericardiocentesis under fluoroscopic guidance. Acta Radiol.33: 309.
- 5.Bastian A, Meissner A, Lins M, Siegel E G, Möller F et al. (2000) Pericardiocentesis: differential aspects of a common procedure. Intensive care medicine. 26(5), 572-6.
- 6.Tsang T S, Barnes M E, Hayes S N, Freeman W K, Dearani J A et al. (1999) Clinical and echocardio graphic characteristics of significant pericardial effusions following cardiothoracic surgery and outcomes of echo-guided pericardiocentesis for management: Mayo Clinic experience. 116(2), 322-31.
- 7.Cheitlin M D, Armstrong W F, Aurigemma G P. (2003) ACC/AHA/ASE guideline for the clinical application of echocardiography.
- 8.Mann D L, Zipes D P, Libby P, Bonow R O. (2014) Braunwald's heart disease: a textbook of cardiovascular medicine: Elsevier Health Sciences;.
- 9.Adler Y, Charron P, Imazio M, Badano L, Barón-Esquivias G et al. (2015) ESC Guidelines for the diagnosis and management of pericardial diseases: the Task Force for the Diagnosis and Management of Pericardial Diseases of the European Society of Cardiology (ESC) Endorsed by: The European Association for Cardio-Thoracic Surgery (EACTS). , Eur Heart J 36(42), 2921-64.
- 10.Maggiolini S, Gentile G, Farina A, De Carlini CC, Lenatti L et al. (2016) Safety, efficacy, and complications of pericardiocentesis by real-time echo-monitored procedure. , Am J Cardiol 117(8), 1369-74.
- 11.Ristić A D, Imazio M, Adler Y, Anastasakis A, Badano L P et al. (2014) Triage strategy for urgent management of cardiac tamponade: a position statement of the European Society of Cardiology Working Group on Myocardial and Pericardial Diseases. Eur Heart. 35(34), 2279-84.
- 12.Maggiolini S, Osculati G, Vitale G. (2005) Utility and safety of diagnostic pericardiocentesis. , Eur Heart J 26(10), 1046-7.
- 13.Cruz I, Stuart B, Caldeira D, Morgado G, Gomes A C et al. (2015) Controlled pericardiocentesis in patients with cardiac tamponade complicating aortic dissection: Experience of a centre without cardiothoracic surgery. Eur Heart J Acute Cardiovasc Care. 4(2), 124-8.
- 14.Standring S, Borley N R, Collins P, Crossman A R, Gatzoulis M A et al. (2008) Gray's Anatomy . London: Churchill Livingstone. 40-978.