
Late Onset Meningitis in Post Traumatic Temporal Meningoencephalocele
Abstract
Temporal lobe meningoencephalocele is an uncommon anomaly in the face. As brain tissue herniate through the dural imperfection, cerebrospinal fluid (CSF) or a mass will appear in the mastoid, middle ear or the both. Here we present a 10 years old boy with right lobe temporal meningoencephalocele which results in CSF leakage and manifested with bacterial meningitis. He had a history of head trauma and bone fracture 3 years ago. In surgery the defect repaired and the patient showed improvement.
Author Contributions
Copyright © 2022 Zahra Sadr, et.al
 This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Competing interests
The authors have declared that no competing interests exist.
Citation:
Introduction
Meningitis is an inflammation of the brain membranes and spinal cord. Bacterial meningitis etiology has been changed in recent decade due to H. Influenza (HIB), S. pneumonia and Meningococcal vaccination 1, 2. It has different risk factors such as; head trauma, immune suppression, central nervous shunts, cerebrospinal fluid fistula/leak, neurological diseases , alcoholism, sinusitis, otitis media, pharyngitis, bacterial pneumonia, sickle cell disease, and congenital defects, age, social factors, exposures to pathogens, immunocompromising factors and drug usage 3, 4, 5, 6, 7 cerebrospinal fluid analysis and culture is the best way for meningitis diagnosis. Some of the most complications that are associated with meningitis is; brain edema, hydrocephalus, infarcts, cerebral herniation and focal infection. They all need cranial CT scan for diagnosis 8.
An encephalocele is a rare congenital neural tube defect. It happens when brain tissues protrude through a hole in the skull. Temporal bone encephaloceles manifest either as a mass or cerebrospinal fluid (CSF) in the middle ear or mastoid or both. Temporal lobe encephalocele is a rare disease. It is estimated about 1/3000 to 1/350009. There are two main etiologies for the temporal lobe encephalocele; acquired (traumatic fracture, radiation, erosions, tumors, etc.) and congenital skull base defects 10. Temporal lobe encephalocele does not have any specific signs and symptoms; so the diagnosis is with delay most of the time. The patient should expect a lot of complications such as seizures, abscess, meningitis and venous infarction, if remain untreated.
Case Report
A 10 years old boy was refered to Rasul Akram Hospital (tertiary hospital) in Tehran, Iran . The clinical presentation was headache, vertigo, and intermediate coughs for one week. The frontal and bitemporal headache intensified by head bending, just one-time fever before admission. He received Co-amoxicalve and diphenhydramine in out-patient. There wasn’t any pain relief by using the drugs and due to the headache worsening and vomiting he was taken to the clinic for serum therapy. His drug was changed to azithromycin. The day after serum therapy he had delirium and gradually leads to loss of consciousness (LOC), was intubated in first hospital, then referred and admitted in PICU of Rasool Akram hospital. In the admission day, he had a fever (39/1), pulse rate=114, respiratory rate=17, blood pressure=116/76. Pupils were in normal size and had reaction to light and his deep tendon reflexes (DTR) were decreased, no kerning or Brudzinski sign. Course crackles in both lungs and downward Babinski reflexes were found in his examination. He was self-extubated about four hours after admission to PICU and was oxygenated by nasal cannula without any decrease in O2 saturation.
Previous History
Three years ago, he had a severe head trauma and skull fracture during car accident and was in coma for 3 months. He gradually improved better and could walk and speak after speech therapy, physiotherapy and occupational therapy.
Findings
Aspiration pneumonia had found in chest CT scan. In addition to blood culture and other laboratory tests, Lumbar puncture had done (without any contraindication in brain Ct scan) CSF analysis determined bacterial meningitis. All the serial laboratory tests showed in Table 1.
Table 1. Results for serial laboratory tests| WBC | 25800 | Neut:86% | Lym:14% | ||||
| 7880 | Neut:57% | Lym:31% | |||||
| 6100 | |||||||
| 6100 | 37% | 43% | |||||
| RBC | 4/14 | 4/83 | 4/5 | ||||
| Hb | 12 | 13/9 | 13 | 12/7 | |||
| Hct | 35/5 | 38 | 39 | ||||
| MCV | 29 | 80 | 86 | ||||
| MCHC | 33 | 35 | 33 | ||||
| Plt | 226000 | 280000 | 405000 | 253000 | |||
| ESR | 31 | 74 | 59 | ||||
| CRP | >48 | >48 | 12 | ||||
| BS | 77 | 82 | |||||
| Na | 136 | 142 | 147 | ||||
| K | 4/8 | 4/4 | 3 | ||||
| Ca | 11/3 | 10/9 | 10/6 | ||||
| P | 2/7 | 4/6 | 4/5 | ||||
| Mg | 2/7 | 2/2 | 1/7 | ||||
| AST | 9 | ||||||
| ALT | 19 | ||||||
| ALK | 375 | ||||||
| BUN | 9 | 14 | 8 | ||||
| Cr | 0/7 | 0/8 | 0/8 | ||||
| CPK | 985 | ||||||
| LDH | 1151 | 519 | |||||
| FERRITIN | 142 | 122 | |||||
| LP | Wbc:6400 | Rbc:1260 | GLU:55 | Pro:210 | LDH:240 | Neut:90% | Lym:10% |
| 10 | 10 | 53 | 13 | 42 | 10% | ||
| CSF/C | negative | Negative | |||||
| U/A | SG:1017 | WBC:10 | RBC:30 | Pro:+1 | Blood:+4 | Bacteria: moderate | |
| SG:1030 | WBC:1-2 | RBC:0-1 | Pro:- | Blood:- | |||
| U/C | negative | Negative | |||||
| B/C | |||||||
| PT | 14/6 | ||||||
| PTT | 29 | ||||||
| INR | ½ | ||||||
| D-dimer | 1317 | ||||||
| ABG | PH:7/38 | PCO2:44 | PO2:27 | HCO3:26 | BE:1/2 | ||
| Covid-19 | PCR | IgM:0/63 | IgG:10/33 |
High dose of Cefotriaxone (100 mg/kg/day) and vancomycin (20mg/kg/q6h) were started. Dexamethasone (0.6 mg/kg/day), Phenytoin (5mg/kg/day/BD), Acyclovir (10mg/kg/dose/TDS) and pneumococcal vaccine, were added. He was clearly alert at second day of admission, and he was transferred to the pediatric ward at third day. His abdominal Sonography was normal. A fracture on the right roof of the right tympan and soft tissue density in the middle ear suggestive cholesteatoma reported in Brain Ct scan on day of admission (Figure 1).
Figure 1.There is evidence of fracture on the right roof of the right tympan. Slight opacity of right mastoid air cells is evident. There is soft tissue density in the middle ear and epitympan and preusak cavity suggestive cholesteatoma.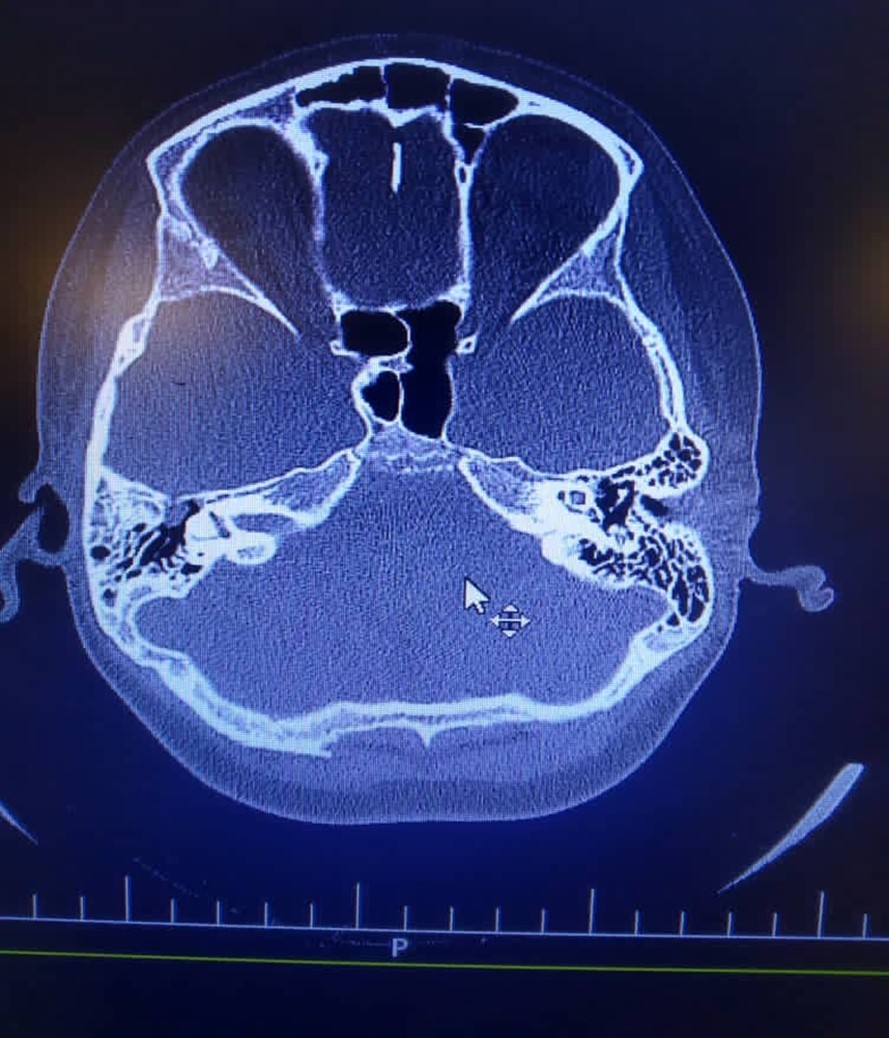
Despite the abnormal manifestation in mastoid cells, the audiometric examination was normal. Due to continuing the headache and right ear, the spiral HRCT of temporal bone without injection was requested. (Figure 2)
Figure 2.High signal intensity in both hemispheres is noted suggestive of meningitis. In T2 sequence there are hyper signal material left maxillary sinuse and bilateral frontal sinuses in favour of sinusitis, polyp and retention cyst in left maxillary sinus is noted. Effusion in right mastoidal air cell is noted.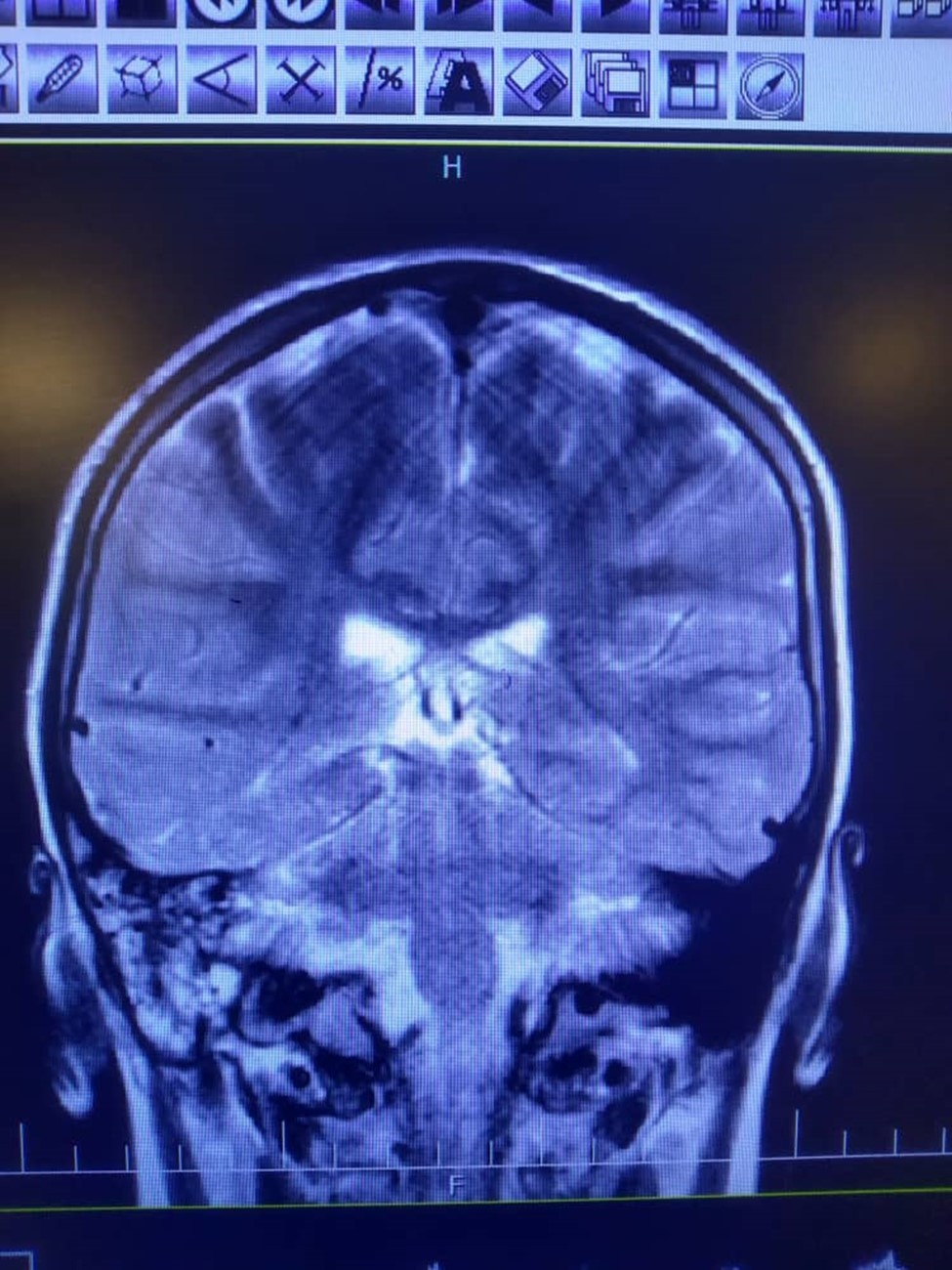
After ten days of treatment, lumbar puncture (LP) was done again which was absolutely normal and his headache relieved more than before. He was discharged, for further visit by ENT and neurosurgeon. Subsequently, after 2 weeks he was admitted by ENT service and was operated. That was an interesting result which was meningoencephalocele of right temporal lobe with CSF leak as detailed below.
ENT surgeon reported: A craniotomy opening is made in the squamous portion of the temporal bone and is approximately 5 cm by 5 cm. This bone flap is based on the root of the zygoma with care to avoid laceration of the underlying dura. The dura is elevated from the floor of the middle fossa. Venous bleeding was controlled with absorbable knitted fabric (Surgical) Dissection of the dura proceeds in a posterior-to-anterior manner. When the dura has been elevated with blunt Dural elevator, the House-Urban retractor was placed on the edge of a bone. The location of the bone defect was observed in anterior medial tegment tympani. The part of the brain tissue that was inside the middle ear was removed. To repair the defect, first a layer of fascia and then a piece of bone was placed on the fascia. Due to the presence of CSF leakage, another layer of fascia was extradural placed on the site of perforation and fixed on the perforated area with the help of fibrin glue. The field is inspected for hemostasis, and the middle fossa retractor is removed, the bony flap was fixed in place by suturing it to the surrounding bones. A mastoid dressing completes the closure.
Our case was visited 2 and 6 months after his surgery without any complications and he had normal hearing.
Discussion
An encephalocele usually happens when brain tissue herniates through a dural defect of the skull. Temporal bone encephaloceles show either as a mass or cerebrospinal fluid (CSF) in the middle ear or mastoid or both.
Cerebrospinal fluid otorrhea and temporal lobe encephaloceles (TLEs) including the tegmen tympani also mastoide are infrequent. neurotologic conditions that have become more common in the past 10 years. 11
Cerebrospinal fluid otorrhea and TLE come with serious aftermaths such as meningitis and brain abscesses, including conductive hearing loss and chronic middle ear effusion. 12
All temporal bone CSF usually occur through the tegmen (tympani or mastoideum) and through the temporal lobe dura. Posterior fossa plate that leak over the cerebellum are not common. 13
CSF leaks that are secondary to head trauma are well documented. It usually resolves spontaneously or with lumbar drainage within 1 to 2 weeks after the incident. 14
Usually, Preparatory radiographic evaluation begins with a high-resolution computed tomography (CT) of the skull base. A magnetic resonance imaging (MRI) study is helpful to display for the presence of an encephalocele and may confirm that the effusion has a similar signal characteristic as CSF. If CT and MRI are non-diagnostic, other imaging formats such as a radionucleotide cisternogram study could be helpful. 15 The gold standard confirmatory test for a CSF fistula is the presence of beta-2 transferrin in the fluid that was used as a sample. 16
A more frequent discovery is a soft compressible mass in the mastoid cavity comming off the tegment that may mimic a blue dome cyst or cholesterol granuloma. 17 Less frequent presentations include meningitis and seizures 1817.
Conclusion
MRI is the gold standard technique for detecting brain tissue herniation in middle ear cavities. The involved tissue is shown as a mass iso-intense in all sequences in MRI. Hypo intense in T1 and hyper intense in T2 with diffusion weighted sequences 25 is seen in cholesteatoma and cholesterol granuloma appears hyper- intense in both T1 and T2. Administration of contrast only will show granulation tissues 24.
CT scan is the other technique for diagnosis. It is so much important to detect the size and location of the involved bones with high resolution computer tomography; but there is a defect with that which cannot detect the solidarity of soft tissues. It has limitation in detecting granulation, cholesteatoma, cholesterol granuloma or other soft tissue masses inside the middle ear cavity. 19, 20, 21, 22, 23
Different surgical techniques now are available. Repairing the whole layers (bone and soft tissue) is more effective than the only repair in soft tissue, due the increased risk of recurrence 25, 26.
Middle cranial fossa craniotomy (MCF), trans mastoid and combined MCF/trans mastoid are one of the surgical techniques for temporal bone CSF-L which reduces the risk of meningitis, conductive hearing loss and otorrhea 27.
Abbreviations
CSF: Cerebrospinal Fluid
HIB: Hemophilus Influenza
PICU: Pediatric Intensive Care Unit
DTR: Deep Tendon Reflexes
LP: Lumbar Puncture
MRI: Magnetic Resonance Imaging
HRCT: High Resolution Compound Tomography
ENT: Otorhinolaryngology
GCS: Glasgow Coma Score
Ethics Approval and Consent to Participate
NA
Consent for Publication
NA
Availability of Data and Materials
NA
Funding
There is no Funding
Acknowledgements
NA
References
- 1.Schuchat A, Robinson K, Wenger J D. (1995) Bacterial meningitis in the United States in. , Active Surveillance Team, N Engl J Med 337, 970-6.
- 2.Dawson K G, Emerson J C, Burns J L. (1999) Fifteen years of experience with bacterial meningitis, PediatrInfect Dis J. 18, 816-22.
- 3.Geiseler P J, Nelson K E, Levin S, Reddi K T, Moses V K.Community-acquired purulent meningitis: A review of 1,316 cases during the antibiotic era, 1954-1976. Rev Infect Dis. 2(5), 725-45.
- 4.Chavez-Bueno S, McCracken GH Jr. (2005) Bacterial meningitis in children. , PediatrClin North Am 52(3), 795-81.
- 6.Schutze G E, Mason EO Jr, Barson W J, Kim K S, Wald E R et al.Invasive pneumococcal infections in children with asplenia. , PediatrInfect Dis J 21(4), 278-82.
- 7.Porto I. (2012) Acute bacterial meningitis. US Pharmacist;. Available from: http:www.uspharmacist.com/continuing_education/ceviewtest/lessoned/108112/
- 8.Beek D Van de, J de Gans, Spanjaard L, Weisfelt M, Reitsma J B et al. (2004) Clinical features and prognostic factors in adults with bacterial meningitis. , N Engl 351(18), 1849-59.
- 9.Golding-Wood D G, Williams H O, Brookes G B. (1991) Tegmental dehiscence and brain herniation into the middle ear cleft. , J Laryngol Otol 105, 477-80.
- 10.Lalwani A K, Jackler R K, Harsh GR 4th, Butt F Y. (1993) Bilateral temporal bone encephaloceles after cranial irradiation. Case report. , J Neurosurg 79, 596-9.
- 11.Nelson R F, Gantz B J, Hansen. (2015) MR: The rising incidence of spontaneous cerebrospinal uid leaks in the United States and the association with obesity and obstructive sleep apnea. , Otol Neurotol 36, 476-480.
- 12.Raine C. (2005) Diagnosis and management of otologic cerebro- spinal uid leak. , Otolaryngol Clin North Am 38, 583-595.
- 13.Kutz JW Jr, Johnson A K, Wick C C. (2018) Surgical management of spontaneous cerebrospinal fistulas and encephaloceles of the temporal bone. , Laryngo- scope 128, 2170-2177.
- 14.Savva A, Taylor M J, Beatty C W. (2003) Management of cerebrospinal fluid leaks involving the temporal bone: Report on 92 patients. , Laryngoscope 113, 50-56.
- 15.Reddy M, Baugnon K. (2017) Imaging of cerebrospinal fluid rhinorrhea and otor- rhea. Radiol Clin North Am. 55, 167-187.
- 16.Warnecke A, Averbeck T, Wurster U, Harmening M, Lenarz T et al. (2004) Diagnostic relevance of beta2-transferrin for the detection of cerebrospinal fluid fistulas. Arch Otolaryngol Head Neck Surg. 130-1178.
- 17.Graham M D. (1982) Surgical management of dural and temporal lobe herniation into the radical mastoid cavity.Laryngoscope. 92, 329-331.
- 18.Ferguson B J, Wilkins R H, Hudson W. (1986) Spontaneous CSF otorrhea from tegmen and posterior fossa defects.Laryngoscope. 96, 635-644.
- 19.Kenning T J, Willcox T O, Artz G J, Schiffmacher P, Farrell C J et al. (2012) Surgical management of temporal meningoencephaloceles, cerebrospinal fluid leaks, and intracranial hypertension: treatment paradigm and outcomes. Neurosurg Focus. 32(6), 6.
- 20.Sanna M, Fois P, Paolo F, Russo A, Falcioni M. (2009) Management of meningoencephalic herniation of the temporal bone: personal experience and literature review. , Laryngoscope 119(8), 1579-85.
- 21.Carlson M L, Copeland W R, Driscoll C L, Link M J, Haynes D S et al. (2013) Temporal bone encephalocele and cerebrospinal fluid fistula repair utilizing the middle cranial fossa or combined mastoid-middle cranial fossa approach. , J Neurosurg 119(5), 1314-22.
- 22.Souliere C R, Langman A W.Combined mastoid/middle cranial fossa repair of temporal bone encephalocele. , Skull Base Surg 8(4), 185-9.
- 23.Leonetti J P, Marzo S, Anderson D, Origitano T, Vukas D D.Spontaneous transtemporal CSF leakage: a study of 51 cases. , Ear Nose Throat J 84(11), 700-702.
- 24.Bovo R, Ceruti S, Padovani R, Martini A. (2006) Temporal bone brain herniation. , Otol Neurotol Off Publ Am Otol Soc Am Neurotol Soc Eur Acad Otol Neurotol 27(4), 576-7.
- 25.B De Foer, Vercruysse J-P, Bernaerts A, Deckers F, Pouillon M et al. (2008) Detection of postoperative residual cholesteatoma with non-echo-planar diffusion- weighted magnetic resonance imaging. Otol Neurotol Off Publ Am Otol Soc Am Neurotol Soc Eur Acad Otol Neurotol. 29(4), 513-7.