Abstract
Lactic acidosis is a condition commonly encountered in the hospital setting particularly in critically ill patients and is very often used as a diagnostic adjunct when encountering cases of ischaemia or other hypoperfusion states. Despite its use many clinicians have long forgotten the biochemical mechanisms that give rise to hyperlactataemia. One reason for this is because the basic science regarding lactate metabolism is taught in the early years of the medical undergraduate course, and unless one specialises in metabolic medicine, is unlikely to encounter it again. In this article we aim to elucidate the basic mechanisms of lactate metabolism and the accompanying acidosis, and illustrate various clinical settings that give rise to this biochemical abnormality.
Author Contributions
Academic Editor: Ramesh C Gupta, Visiting Professor, National Institute of complementary Medicine (NICM) University of Western Sydney Australia
Checked for plagiarism: Yes
Review by: Single-blind
Copyright © 2016 Sanjay Harrison, et al.
 This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Competing interests
The authors have declared that no competing interests exist.
Citation:
Introduction
Lactic acidosis is a condition commonly encountered in the hospital setting particularly in critically ill patients and is very often used as a diagnostic adjunct when encountering cases of ischaemia or other hypoperfusion states. Despite its use many clinicians have long forgotten the biochemical mechanisms that give rise to hyperlactataemia. One reason for this is because the basic science regarding lactate metabolism is taught in the early years of the medical undergraduate course, and unless one specialises in metabolic medicine, is unlikely to encounter it again. In this article we aim to elucidate the basic mechanisms of lactate metabolism and the accompanying acidosis, and illustrate various clinical settings that give rise to this biochemical abnormality.
Types of Lactic Acidosis
Lactic acidosis has traditionally been accepted to be defined as serum lactate concentration of 5 mmol/L with a pH of 7.35 or less. Cohen and Woods have divided lactic acidosis into type A and type B which differ with respect to the presence or absence of hypoperfusion and poor tissue oxygenation (table 1).1 A more recent review by Kruse et al characterise normal lactate levels as less than 2 mmol/L, intermediate lactate levels as between 2 mmol/L and 4 mmol/L and high levels as being 4 mmol/L or more.2
Table 1. The classification of lactic acidosis according to the underlying etiolog| Type | Features | Aetiology |
| A | Hypoperfusion | Increase in production or decrease in excretion of lactate e.g. shock, ischaemia and liver disease |
| B | No hypoperfusion | B1 Systemic disease e.g. diabetes, renal failure, some malignancies |
| B2 Medications e.g. biguanides, isoniazid, salicylates and ethanol | ||
| B3 In-born errors of metabolism e.g. pyruvate dehyrogenase deficiency, pyruvate carboxylase deficiency and MELAS |
In type A lactic acidosis there is an accompanying hypoperfusion and poor tissue oxygenation and the hyperlactataemia is the consequence of increased production or reduced clearance of lactate. This type of lactic acidosis is commonly seen in conditions such as shock, ischaemia and liver disease.
Type B lactic acidosis occurs when there is no clinical evidence of hypoperfusion and has been subdivided into three different categories according to the etiology.
Type B1 lactic acidosis is the consequence of systemic diseases such as diabetes, renal failure and can also occur in certain malignancies.
Type B2 lactic acidosis is the result of certain medications and is usually iatrogenic. Notable causative agents include biguanides, isoniazid, alcohol and salicylates.
Type B3 lactic acidosis arises from genetic mutations that result in errors in metabolism. This is congenital and includes conditions such as pyruvate dehydrogenase deficiency, pyruvate carboxylase deficiency and MELAS (mitochondrial encephalomyopathy, lactic acidosis and stroke like episodes).
Lactate and H+ Generation
Glycolysis, which occurs in the cytoplasm of every cell results in the formation of pyruvate as an end product. In an aerobic environment, the pyruvate enters the mitochondria and passes through the Krebs cycle. This results in the generation of ATP and CO2 and H2O as end products.
In an anaerobic environment, pyruvate gets converted to lactate by the action of lactate dehydrogenase. This process requires the reduced form of nicotinamide adenine dinucleotide (NADH). An anaerobic environment increases the NADH/NAD+ ratio which favours the formation of lactate. As pyruvate gets shunted towards the formation of lactate, the normal ratio of lactate to pyruvate increases from its normal value of approximately 20:1.3
The generation of lactate via the shunting of pyruvate in an anaerobic environment results in a relatively low yield of 2 moles of ATP for every mole of glucose. Hydrolysis of ATP occurs as per the equation;
In aerobic environments, the products are re-used to re-constitute ATP. In aerobic environments, these products accumulate and it is this reaction rather than the lactate per se that results in the generation of H+ ions and the subsequent acidosis.4
Lactate is also produced by the liver, kidneys, lung and skeletal muscle in various pathological states and accumulates once the production overwhelms the body’s clearance mechanisms (figure 1).5
Figure 1.A schematic depiction of the metabolism of lactate and the various factors that influence it.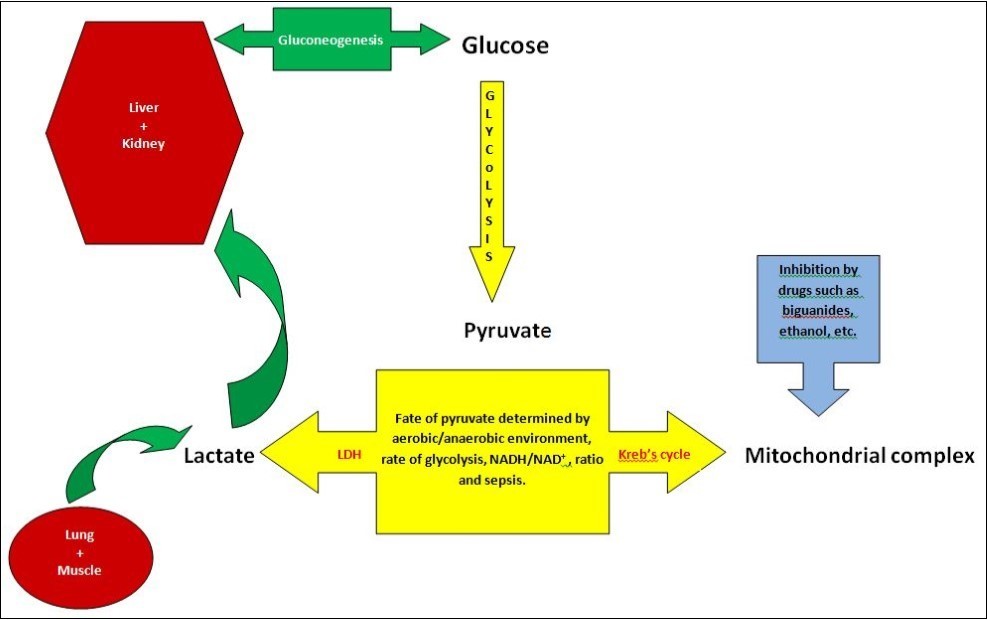
Lactate Clearance
The liver is primarily responsible for the clearance of lactate from the blood. It has been estimated that between 50%-70% of the lactate is cleared by the liver.3, 6 While lactate is freely filtered through the glomerulus of the kidney, the majority of it is re-absorbed in the proximal tubules with very little being excreted. Lactate clearance by the kidney is primarily by metabolic processes such as gluconeogenesis. Lactate produced by other organs in the body are transported back to the liver and are converted back to glucose (Cori cycle).3
Lactic Acidosis in Sepsis/SIRS
While in many cases of sepsis, the high lactate levels are due to poor tissue perfusion, type B lactic acidosis has also been seen to occur. While large scale studies are lacking, many experiments in animals and humans have implicated increased pyruvate production, decreased pyruvate dehydrogenase (PDH) activity, lactate production from the lung and decreased lactate clearance as causative mechanisms.
A study on 5 septic patients and 6 controls by Gore et al utilised isotope tracer techniques and demonstrated that septic patients produce higher levels of pyruvate.7 Studies of experimental models of sepsis by Vary et al have demonstrated that PDH kinase activity is enhanced during sepsis which inactivates the PDH molecule.8 This leads to increased pyruvate being shunted towards lactate production. Severin et al demonstrated decreased clearance of lactate in animal models of sepsis.9 Their results were backed by the work of Chrusch et al who also demonstrated decreased lactate clearance in animal models of sepsis in addition to increased splanchnic production.10 Kellum et al in a study of 9 patients and 12 controls demonstrated that lactate production is increased in acute lung injury which according to them could partly explain the hyperlactatemia seen in sepsis.11 A prospective study of 70 patients by Routsi et al showed similar results, with the observed hyperlactatemia not attributable to lung tissue hypoxia.12
Lactic Acidosis in Bowel Ischaemia
Lactate levels are checked by Surgeons when encountering cases of bowel ischaemia. Lactic acidosis occurs in bowel ischaemia as a consequence of hypoperfusion, however what must be emphasised is that hyperlactatemia is a late occurrence and is therefore not useful in diagnosing ischaemia early. The time required for bowel ischaemia to result in hyperlactatemia is variable and has been estimated from animal studies. A study done by Kurimoto et al looked at serial measurements of various acidosis related serological markers taken from different blood vessels of an anaesthetised pig which had its superior mesenteric artery (SMA) ligated.13 Only the serum lactate level from the superior mesenteric vein (SMV) was noted to increase within one hour of SMA ligation. Acidosis related variables only showed significant changes after 4 hours from the other blood vessels. Acosta el at (2007) performed a similar study on surgically induced SMA occlusion in 9 pigs with 6 controls.14 Their results did not demonstrate any significant rise in plasma lactate between the two group even after 6 hours of ischaemia. They conclude that serum lactate levels are not useful as an early marker of intestinal ischaemia. These studies provide an experimental basis for the observation that patients have been found to have ischaemic bowel on laparotomy but have had normal lactate levels which were measured earlier. The delay between the onset of bowel ischaemia and hyperlactatemia may be attributable to the time required for the hepatic clearance mechanisms to be overwhelmed or fail.
Drug Induced Hyperlactatemia
Various drugs have been implicated in the development of lactic acidosis, most notably the biguanides.15 While reports of metformin induced lactic acidosis are rare, it was more commonly noted in the similar drug phenformin which is no longer in use. While these drugs enhance glucose uptake and metabolism, they also inhibit gluconeogenesis and complex I of the mitochondrial respiratory chain.16, 17 Nucleoside reverse transcriptase inhibitors (NRTIs) are known to produce adverse effects on mitochondria which can result in lactic acidosis in addition to hepatic steatosis, myopathy and neuropathy.18
Ethanol intoxication results in hyperlactaemia and can precipitate the development of acidosis.19Ethanol is metabolised by alcohol dehydrogenase and then aldehyde dehydrogenase which generates NADH in the process. The generation of NADH alters the NADH/NAD+ ratio which results in the conversion of pyruvate to lactate.
Lactic Acidosis in Malignancy
Both types of lactic acidosis have been reported in cases of various malignancies. Type A occurs as a result of hypoperfusion however type B is due to a variety of causes. Very often, it results from the use of medications, an increased tumour burden or even decreased lactate clearance due to hepatic involvement. Cancer cells are also known to have increased glucose requirements (Wittig et al) and increased glycolytic activity.20 The intermittent tissue hypoxia experienced by malignant tissue stabilises the hypoxia inducible factor (HIF-1) which in turn activates pyruvate dehydrogenase kinase (PDH kinase). This enzyme inactivates PDH which contributes to the generation of lactate.
Thiamine Deficiency
In addition to deficient lactate clearance, hyperlactataemia can also arise as a result of defects in the biochemical components of the cellular oxidative machinery. The PDH complex which converts pyruvate to acetyl coA has various co-factors which includes thiamine pyrophosphate. A lack of the appropriate co-factor would impair the normal aerobic processes and result in the generation of lactate. In a clinical context, such a scenario is commonly encountered in patients with hyperlactataemia who also have a thiamine deficiency due to poor nutritional intake. This commonly occurs in alcoholic patients and would therefore also contribute to the hyperlactataemia seen in such patients. Shah et al report the case of a paediatric patient presenting with hyperlactataemia due to a lack of thiamine in the patient’s total parenteral nutrition which did not resolve until the administration of thiamine.21 A similar case is also reported by Da Silva et al where a patient with persistent hyperlactataemia and parenteral nutrition dependent was found to be thiamine deficient.22
D-Lactic Acidosis
D-lactate is the product of the bacterial metabolism of starch, sugar and undigested fibre within the gut and is not produced by any of the human organs. The accumulation of D-lactate occurs in patients with short bowel syndrome or in patients who have undergone bypass surgery for morbid obesity. This condition is associated with a metabolic acidosis and neurological symptoms, however because laboratory assays are specific for L-lactate, the diagnosis is commonly missed. The intraluminal pH changes that accompany the condition favours the proliferation of Lactobacillus within the gut which is one of the main D-lactate producing bacteria.23
Managing the Patient with Hyperlactataemia
Among the myriad causes of hyperlactataemia, sepsis and visceral ischaemia (eg acute ischaemic bowel) are the most serious and therefore the clinician should take appropriate steps to establish whether the hyperlactataemic patient (type A hyperlactataemia) has either of these conditions. States of hypoperfusion would require adequate resuscitation and prompt therapeutic intervention according to standard protocols. In the event of suspected ischaemic bowel, the patient if fit enough, would require surgical intervention. Very often, adequate fluid resuscitation would result in an improvement of the hyperlactataemia and any accompanying acidosis. Once these conditions have been ruled out and the patient is found to be sufficiently well perfused, a cause for the type B hyperlactataemia must be sought. This would entail a thorough and detailed history taking from the patient and must include a drug history and any other associated symptoms.24
The prognostic significance of elevated lactate levels vary according to the clinical context. For example, it is well established that elevated lactate levels in the clinical context of a septic patient is a poor prognostic indicator. Although elevated lactate levels may be seen in patients post epileptic seizures or asthma attacks, there is no evidence to suggest it has any bearing on the clinical outcome. Given the multifactorial aetiology of hyperlactataemia, it is important for the clinician to be mindful of the fact that very often there may be several factors contributing to hyperlactataemia in a patient and therefore the approach in managing such patients should be aimed at identifying and addressing all relevant possible causes.24, 25
Summary
Lactic acidosis is typically defined as a pH of < 7.35 in the presence of a lactate of > 5 mmol/L and is broadly divided into type A and type depending on the presence or absence of hypoperfusion and decreased oxygenation. Contrary to popular belief, the acidosis is the result of the hydrolysis of ATP and not the dissociation of the lactic acid molecule. The clinical insights gained from an understanding of the metabolism of lactate are numerous. Such knowledge would aid the clinician in interpreting the results of serum lactate measurements especially when encountered with diagnostically challenging cases such as mesenteric ischaemia.26 Lactate levels begin to rise only when the clearance mechanisms become overwhelmed which would be due to critical illness or over production of lactate. As hyperlactatemia is usually encountered in critically ill patients, much of our understanding derives from animal studies and limited human studies. Nevertheless, many of these results have and can be extrapolated to find applications in clinical practice. While ischaemia and sepsis are common causes, clinicians must be aware that hyperlactatemia with acidosis may also be the results of medications such as biguanides, salicylates and NRTIs.
Key Points
Lactic acidosis can occur in the presence (type A) or absence (type B) of hypoperfusion and poor oxygenation
The acidosis is the consequence of the hydrolysis of ATP and not the lactic acid molecule
Hyperlactatemia is a late sign in bowel ischaemia
While commonly encountered in the critically ill patient, lactic acidosis can also be the consequence of certain medications such as biguanides, salicylates, alcohol, congenital errors in metabolism and even certain malignancies.
References
- 1.Cohen R D, Woods H F. (1976) Clinical and biochemical aspects of lactic acidosis. Osney Meade, Oxford,UK;Blackwell Scientific;.
- 2.Kruse O, Grunnet N, Barford C. (2011) Blood lactate as a predictor for in hospital mortality in patients admitted acutely to hospital : a systematic review.ScandJTraumaResuscEmergMed19-74.
- 3.Fall P J, Szerlip H M. (2005) Lactic acidosis: From sour milk to septic shock.J Intensive Care Med20:. 255-271.
- 4.Robergs A, Ghiasvand F, Parker D. (2004) . Biochemistry of exercise induced metabolic acidosis.Am JPhysiolRegulIntegrCompPhysiol287: R 502-R 516.
- 6.Phypers B, Pierce J M. (2006) . Lactate physiology in health and disease.ContinEducAnaesthCritCare Pain6(3): 128-132.
- 7.Gore D C, Jahoor F, Hibbert J M, DeMaria E J. (1996) Lactic acidosis during sepsis is related to increased pyruvate production, not deficits in tissue oxygen availability.AnnSurg244(1):. 97-102.
- 8.Vary TC.(1996Aug) Sepsis induced alterations in pyruvate dehydrogenase complex activity in rat skeletal muscle: effects on plasma lactate. , Shock 6(2), 89-94.
- 9.Severin P N, Uhing M R, Beno D W. (2002) Endotoxin induced hyperlactatemia results from decreased lactate clearance in hemodynamically stable rats.CritCare Med30:. 2509-2514.
- 10.Chrusch C, Bands C, Bose D. (2000) Impaired hepatic extraction and increased splanchnic production contribute to lactic acidosis in canine sepsis.Am JRespirCritCare Med161:. 517-526.
- 11.Kellum J A, Kramer D J, Lee K. (1997) Release of lactate by the lung in acute lung injury.Chest111:. 1301-1305.
- 12.Routsi C, Bardouniotou H, Delivoria-Ioannidou V. (1999) Pulmonary lactate release in patients with acute lung injury is not attributable to lung tissue hypoxia.CritCare Med27(11):. 2469-2473.
- 13.Kurimoto Y, Kawaharada N, Ito T. (2008) An experimental evaluation of the lactate concentration following mesenteric ischaemia.SurgToday38(10):. 926-930.
- 14.Acosta S, Nilsson T K, Malina J. (2007) L-lactate after embolisation of the superior mesenteric artery.JSurgRes143(2):. 320-328.
- 15.Liamis G, Milionis H J.Elisaf M.(2010) Pharmacolgically induced metabolic acidosis: a review.DrugSaf33(5):. 371-391.
- 16.Owen M R, Doran E.Halesrtap AP.(2000) Evidence that metformin exerts its anti-diabetic effects through inhibition of complex 1 of the mitochondrial respiratory chain.BiochemJ348(3):. 607-614.
- 17.Lalau JD.(2010Sep1).Lactic acidosis induced by metformin: incidence, management and prevention. , Drug Saf; 33(9), 727-740.
- 18.Claessens Y E, Chiche J D, Mira J P. (2003) Bench to bedside review: severe lactic acidosis in HIV patients treated with nucleoside analogue reverse transcriptase inhibitors.CritCare7(3):. 226-232.
- 19.Gauthier P M.Szerlip HM.(2002).Metabolic acidosis in the intensive care unit.CritCareClin18(2):. 289-308.
- 20.Wittig R, Coy J F. (2008) The role of glucose metabolism and glucose associated signalling in cancer.PerspectMedicinChem18(1):. 64-82.
- 21.Shah S, Wald E. (2015) Type B lactic acidosis secondary to thiamine deficiency in a child with malignancy.Pediatrics135(1):e221-e224.
- 22.Da Silva YS, Horvat C M.Dezfulian C.(2015 Jul)Thiamin deficiency as a cause of persistent hyperlactatemia in a parenteral nutrition dependent patient. , J Parenter Enteral Nutr 39(5), 604-606.
- 24.Andersen L W, Mackenhauer J, Roberts J C.(2013October) Etiology and therapeutic approach to elevated lactate. , Mayo Clin Proc 88(10), 1127-1140.