
Abstract
Cerebral aspergillosis is a severe disease most commonly suspected in immunodeficient patients.
The objective of this study is to determine the role of surgery in management of intracranial aspergillosis. We report three cases of immunocompetent patients presenting: posteriror fossa aspergillosis, sphenoidal extended to sellar region aspergillosis and post operative aspergillosis without extracerebral involvement. Microbiology and histological examination were carried out to provide the diagnosis. The patients underwent surgical procedure associated with medical treatment or not. In one case, surgical treatment was efficient. The outcome was good in two cases.
Conclusion:
Rapid diagnosis of invasive aspergillosis applying radiological and surgical procedures and immediate ignition of antifungal can be life saving.
Author Contributions
Academic Editor: Mourad Tayebi, The University of Surrey
Checked for plagiarism: Yes
Review by: Single-blind
Copyright © 2017 K Quenum, et al.
 This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Competing interests
The authors have declared that no competing interests exist.
Citation:
Introduction
Cerebral aspergillosis is severe parasitic disease which is rare in immunocompetent individual. The invasive form with multiple visual involvements is usually seen with immunosuppression. New therapeutic agents such as voriconazole and capsofungine which are more save and efficacious have changed the outcome of this fatale cerebral infection.
Case 1
A 47 year old patient with no previous medical history presented with features of raised intracranial pressure, statokinetic cerebellar syndrome as well as left sided hemiparesis. The diagnosis of posterior fossa space occupying lesion was made. Neuroradiologic investigations demonstrated posterior fossa lesions. Magnetic resonance imaging and spectroscopy were in favor of a multiple infective process (Figure 1). Stereotatic biopsy was carried out on the patient and parasitological and histological examinations of the specimen concluded to a filamentous fungal infection of Aspergillus type. Culture and staining techniques categorized the specie as Aspergillus fumigatus (Figure 2).
Figure 1.cerebral MRI axial T1-weighted (A) and coronale (B), showing a multiples well circumscribed posterior fossa lesions
Figure 2.( A) filamentous fungal infection of Aspergillus type. (B) Culture and staining techniques categorized the specie as Aspergillus fumigatus
Patient was placed on intra veinous amphotéricin B but this was complicated with acute active hydrocephalus warranting external ventricular drainage (Figure 3). Subsequently, he developped staphylococcal meningitis as day 8 post op, treated with intra veinous vancomycin. Patient developed renal insufficiency and hyperosmolar non ketotic coma for an unknown diabetis for which amphotéricine B therapy was stopped. His neurological status deteriorated with a Glasgow coma scale (GCS)7/15. Posterior fossa surgery was performed with excision of the fungal abscess (Figure 4) and Voriconazol was instituded post operatively for fungal therapy with improvement of the neurological status to GCS 13/15. But the patient succumbed to acute cardiac failure.
Figure 3.cerebral CT scan with axial view showing acute hydrocephalus (A) and control after external ventricular drainage (B)
Figure 4.cerebral CT scan pre operative (A) and post operative (B) after posterior fossa surgery with total removal or abscesses
Case 2
A 65 year-old man presented with progressive visual decrease and ptosis in the left eye. Neurological examination revealed paresis of the 3rd left cranial nerve. Fundoscopy revealed bilateral papillary paleness and visual acuity was: 4/10 at left; 7/10 at right. No signs of endocrine insufficiency or hypersecretion were assessed. There was no evidence of sinusitis. Chest X-ray, routine laboratory investigations and hormonal blood tests were normal. A CT scan showed a hypodense mass enlarging the sphenoid sinus and sellar region with calcification like images and bone erosion of the sellar floor (Figure 5). MRI showed a mass of 26 mm x 33 mm x 25 mm in the sphenoidal sinus ans sellar region, with hypersignal intensity in T1-weighted (Figure 6A) ans T2-weighted sequences, and hyposignal zone in T2-weighted sequences (Figure 6B). Imaging investigations were suggestive of unusual pituitary macroadenoma. The patient underwent a transnasal transsphenoidal approach for excision of the mass. A yellow-brownish gluey material with gummy debris was aspirated from the sphenoid sinus, which was completely cleaned. The sellar floor was eroded which allowed a view of the intact inflammatory dura. An intra-operative presumptive diagnosis was made of caseating granuloma (i.e tuberculosis). The post-operative course was uneventful: the patient recovered from ptosis and visual acuity improve at discharge. Mycobacterium tuberculosis could not be cultured from specimens; and cultures on Sabouraud’s medium did not isolate Aspergillus. Pathologic findings were of non invasive aspergillosis, with many septated fungal hyphae being present without tissue invasion. The patient was not given antifungal drugs because the intrasphenoidal material was completely aspirated. At 6 month and 18 months follow up, the patient had no neurological complaint. No recurrence was observed on control CT scans.
Figure 5.CT scan showing a hypodense mass enlarging the sphenoid sinus and sellar region with calcification like images and bone erosion of the sellar floor
Figure 6.(a) Sagittal T1-weighted MRI showing a well circumscribed hyperintense process in the sphenoidal sinus and sellar region; (b) parasagittal T2-weighted MRI showing a regular hypointense zone into the hyperintense process which is specific to aspergillus infection and corresponds to iron accumulation
Case 3
A 45 year-old woman, operated 6 months before for left sphenoid wing meningoma revealed by raised intracranial pressure, with hemiplegia. She underwent surgery, with simpson I resection. The post operative outcome was good and the patient was discharge. Six months later, she presented a swelling on surgical site of skin incision. Blood check found inflammation with raised C-Reactive Protein. CT scan permitted to suggest brain abcess and she was operated in emergency with bone flap removal and the abscess complete excision. Bacteriologic and Histologic examination of the pus, revealed aspergillus flavius. The patient was treated by amphotéricin B because it was the antifungal avalailable in the hospital officine. Two months treatment was necessary to controle cerebral aspergillosis (Figure 7) and the patient was discharged with good outcome.
Figure 7.(A) pre operative MRI, axial T1 weighted with enhancement of sphenoid wing meningioma. (B) Ct scan showing an brain abscess in post op area. (C) CT scan after remoral sugery and 2 months medical treatment.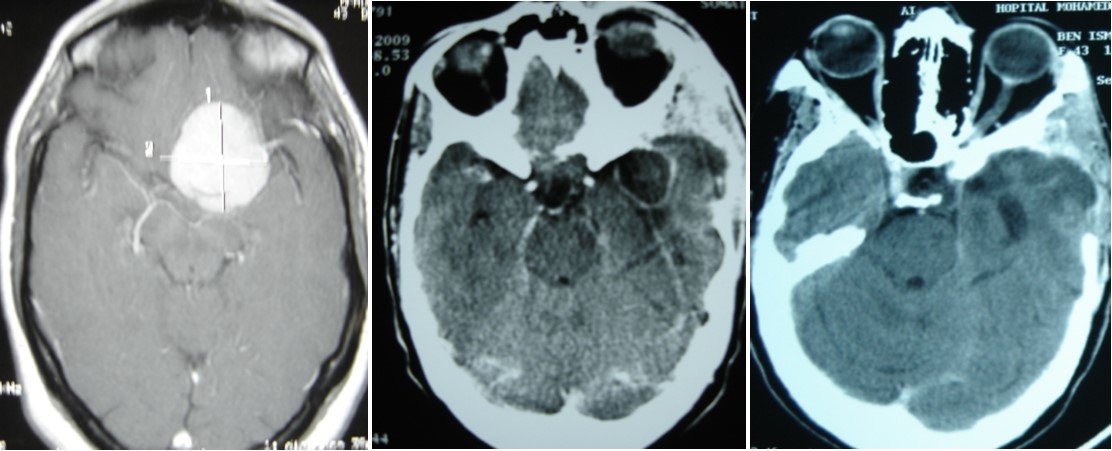
Discussion
Cerebral aspergillosis is one of the common sites secondary to invasive aspergillosis from hematogenous dissemination 1, 8 or contignous spread aspergillus from paranasal sinuses 2, 3. Pulmonary involvement is rarely seen in immunocompetent patient unlike the immunosuppressed. The quest for blood supply especially the thalamic perforators explains its localizations around the substancia nigra. Posterior fossa lesions without other sites are rare, like in our case 1. The clinical presentation is that of a posterior fossa space occupying lesions. Supra tentorial lesions are pleomorphic. They may present with functionnal neurological syndrome or raised intracranial pressure with sepsis syndrome. Risks factors for cerebral aspergillosis in an immunocompetents patients described in literature include old age, diabetes, alcoholism, illicit drug abuse and brain surgery like case 3 6, 9. Our patient case 1, presented with undiagnosed diabetes which was confirmed on admission. Brain CT scan with contrast may not suggest the diagnosis because the lesions are not located in the substancia nigra 6. Only MRI with spectroscopy could suggest an infectious process rather than tumour. This indicated stereotatic biopsy in our patient as a first step followed by bacteriological and histological examinations of the specimen which confirmed the diagnosis. Amphotéricin B is the reference drug in our department for its efficacy, availability and cost. Voriconazol was substituted because of the sides’ effects in our patient. Side effect are well known draw backs of amphotéricin B therapy. With introduction of vancomycin for treatment of post op staphylococcal meningitis, renal failure was the consequence of its toxicity, warranting the stoppage of the therapy. But with neurological deterioration our patient was operated upon with excision of the focus of infection in the posterior fossa, duro plasty and introduction of voriconazol.
In the literature, surgery was indicated in compressive (symptomatic) lesions or for diagnostic biopsy 3, 5, 8.
The treatment of choice for sino-orbital aspergillosis or sphenoidal is surgical excision of the aspergilloma, granulation tissue of the involved sinus for ventilation and drainage, as early as possible 1, 5, 7, 8. Furthermore, there was shown a beneficial effect of pre-surgical treatment with antifungal therapy 9, 10. In patients for whom total removal cannot be achieved, intensive therapy with antifungal agents must be started immediately. But for the case 1, pre operative medical treatment was not satisfactory.
For the patient 3, it should be noted that all bacteriological samples performed in the theatre especially to identify nosocomial risks are unsuccessful.
Conclusion
Cerebral aspergillosis is a serious disease; the diagnosis of which should be suspected in case of immunosuppression with search for primary focus in the lungs or paranasal sinuses. Therapy with antifungal agents still remain delicate. Surgical removal of sphenoid sinus aspergillosis cases proved to be efficient. Other sites infections must be completed by antifungal treatment 4
References
- 1.Boutarbouch M, Arkha Y, A El Ouahabi, S. (2009) Derraz, A El khamlichi. Sphenoid aspergillosis simulating pituitary tumor in immunocompetent patient. , J. Clin Neurosci 16(6), 840-41.
- 2.Kawakami N, Nishizaki T, Sugiyama S. (1994) aspergillus brain abscess in a patient with normal immunity. , Neurol Med Chir (Tokyo) 34, 234-40.
- 3.Louati I, Zaouali J, Azzouz O, Sellami A. (2009) aspergillose cérébrale chez le sujet immunocompétent. A propos de trois cas. Neurol-324; 5
- 4.Wasaya Mohammad, Azam Junaid Patel Iqbal, Muhammad Aslam Khana, Jr Raymond A Smego. (2009) Preoperative antifungal therapy may improve survival in patients with Aspergillus brain abscess Clinical Neurology and. , Neurosurgery 111, 565-567.
- 5.Panda N K, Saravanan K, Chakrabarti A. (2008) Combination antifungal therapy for invasive aspergillosis: can it replace high-risk surgery at the skull base?. , Am J Otolaryngol 29, 24-30.
- 6.Phuttharak W, Hesselink J R, Wixon C. (2005) MR features of cerebral aspergillosis in an immunocompetent patient: correlation with histology and elemental analysis. , AJNR Am J Neuroradiol 26, 835-8.
- 7.Siddiqui A A, Shah A A, Bashir S H. (2004) Craniocerebral aspergillosis of sinonasal origin in immunocompetent patients: clinical spectrum and outcome in 25 cases. , Neurosurgery 55, 602-13.
- 8.Tattevin P, Jauréguibbery S, Gangneux J P. (2004) Les aspergilloses cérébrales. , Rev Neurol (Paris) 160, 597-605.