
Dental Sinus Infections- Why are we Still Missing the Well Documented Diagnosis?
Abstract
Background:
Dental infections, salivary gland lesions, neoplasms and developmental abnormalities can cause oral cutaneous fistulae, fistulae of the neck and intraoral fistulae. Published case reports deliver the same message; that these lesions are misdiagnosed and treated late and ineffectively and this remains a significant on-going problem.
Aim:
It is important to reiterate the management and diagnosis of this condition, despite the fact that it is already well documented in the current literature as patients are still being subjected to unnecessary treatment.
Design and Setting:
We performed a retrospective review of 5 consecutive dental sinus infections between June 2013 and January 2014 that were misdiagnosed initially. Information was extracted from the medical case notes of 2 male and 3 female patients with an age range from 12-87 years.
Method:
The medical records of all 5 patients were analyzed, medical photography was taken and the patients were followed up regularly in our clinic.
Results:
Each patient presented with a non-healing lesion and all were treated with either oral or topical antibiotics. Patients were eventually referred to the craniofacial department where they all received an orthopantomogram and underwent dental extraction, which led to complete healing.
Conclusion:
Cutaneous facial sinus tracts of odontogenic origin are often initially misdiagnosed which leads to prolonged and inappropriate treatment. Correct diagnosis and treatment will result in predictable and rapid healing and thus it is essential to record these case series, to ensure that medical professionals are aware of the presenting symptoms, which can often be very subtle.
Author Contributions
Academic Editor: Ioannis Chatzistefanou, Oral and Maxillofacial Department of the 401 General Military Hospital of Athens
Checked for plagiarism: Yes
Review by: Single-blind
Copyright © 2017 Florian Bast, et al
 This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Competing interests
The authors have declared that no competing interests exist.
Citation:
Introduction
Dental infections, salivary gland lesions, neoplasms and developmental abnormalities can cause oral cutaneous fistulae, fistulae of the neck and intraoral fistulae. Odontogenic cutaneous sinus tracts are a rare, but well documented condition. There have been numerous published case reports on this condition with extra focus given to diagnostic information and management strategies. More often than not, the literature delivers the same message; that the lesions are diagnosed incorrectly and thus treated late and ineffectively. The cutaneous tracts tend to occur more frequently as a result of infected mandibular teeth (80%) more than infected maxillary teeth (20%) 1, 2, 3, 4, 5, 6, 7, 8.
Often, the first presentation of a dental sinus infection is a chronic, inflamed and poorly healing wound in the submental area or on the lower border of the mandible. Usually, patients are referred after unsuccessful oral antibiotic therapy for further treatment. They undergo multiple surgical excisions or biopsies which cause unnecessary scarring, further courses of antibiotic therapy, and even occasional radiotherapy with eventual recurrence of the cutaneous sinus tract and all because the primary dental cause is frequently misdiagnosed. However, if the correct diagnosis of the sinus tract is identified, the problem can be managed with a simple and effective treatment that comprises removal of the infected pulp canal tissue, which subsequently results in minimal cutaneous scarring 2, 3, 5, 6, 8, 9, 10.
Sinus tracts may result from localised infections, such as an infected tooth, periodontal disease, actinomycosis or osteomyelitis. The most common cause of a cutaneous sinus tract is a chronic dental periapical infection or a dentoalveolar abscess. Periapical dental infections can lead to chronic osteomyelitis, cellulitis, and facial abscesses and infection can spread through the skin by taking the path of least resistance. These abscesses arise from bacterial invasion, chemical irritation, or trauma and the most common initiating factor of the periradicular abscess is carious exposure and subsequent bacterial invasion of the tooth pulp. With these causes in mind, the first logical step if a dental sinus is suspected, should be the referral to a dentist or maxillofacial surgeon for further investigation and subsequent management. Several articles have been published on the late diagnosis and mistreatment of dental sinus infections in dental, maxillofacial and dermatology literature, but very few in general medicine, which is perhaps why the diagnosis is still being missed so frequently by general practitioners 6, 11, 12, 13, 14. Therefore, it is important to reiterate the management and diagnosis of this condition, despite the fact that it is already well documented in the current literature as patients are still being subjected to unnecessary treatment. The cases documented here in our article were wrongly originally referred to the dermatologists and the ear nose and throat (ENT) department at our institute and only after a delayed time period, an in-house referral was made correctly to the craniofacial unit.
Method
Clinical Diagnosis
The clinical diagnosis of an infected dental sinus tract requires a thorough history and an appreciation for the fact that any cutaneous lesion of the face and neck could be of dental origin, even without any accompanying dental symptoms, such as pain. After the medical history is ascertained, a systematic clinical examination is necessary, including bimanual palpation of the oral cavity. Purulent discharge while palpating around the skin lesion confirms the presence of a septic tract. According to Stoll et al. the most characteristic feature of the nodule is its “depression or retraction below the normal surface, which is caused by the fixation of the tract with the underlying tissues and may be secondary to the healing process or a late finding in active disease” 15. Often these lesions are also surrounded by scar tissue as they have been previously biopsied or a surgical removal or radiotherapy has been performed 6, 7, 14.
Intraoral findings on examination typically include poor dental hygiene with one or more severely decayed teeth or a healthy looking tooth with an intact crown or slight fracture of the crown. If we felt it was necessary, we would also look at the response of the infected tooth to hot and cold stimuli.
In general, it is not necessary to trace the sinus tract from the cutaneous orifice to the point of origin with a lacrimal probe. However, tracing the tract during radiology imaging, with the probe in-situ, can often be of enormous diagnostic benefit as it can show the origin of the problem directly. If the probe is not in situ, an orthopatomogramm (OPG) will reveal periapical radiolucencies associated with the affected tooth. An ultrasound examination of the lesion can also be performed as part of the diagnostic process. Usually, a computed tomography (CT) scan or ConeBeam is not necessary, however, two of the patients documented in this paper had received a CT scan prior to their referral to our department.
Treatment
Treatment for this condition consists of a root canal treatment or extraction of the affected tooth.A tooth that has significant tissue damage and is non-restorable should normally be extracted. Otherwise, a root canal is the preferred treatment. Microbiology specimens for culture and sensitivity should be sent of any exudate. In addition, cultures should also be sent for suspected fungal or syphilitic infections. We also performed histopathological examinations of a biopsy taken from the cutaneous side of the tract. After the extraction or root canal surgery, healing of the face or neck lesion and tract usually occurs within the first 2 weeks. The area can heal with a slight dimpling and hyperpigmentation but improves with massaging and moisturising using a water based cream during the day and a silicon cream before going to bed, in the upcoming months.
All of our patients were advised to keep excellent oral hygiene by brushing their teeth twice per day and using Chlorhexidine mouth wash in addition to a soft diet for 10 days.
Review
A retrospective review of 5 consecutive cases treated using this technique was performed. Information extracted from the medical case notes included demographic data, defect classification, surgical procedure, complications, and recurrence of a fistula. Aesthetic outcome was assessed by the patient and surgeon satisfaction at clinical follow-up.
Results
Five patients underwent the described procedure between June 2013 and January 2014. Below is a summary Table 1 of the 5 cases, followed by a more detailed outline of each case.
Table 1. Summary| Patient | age | gender (M/F) | Presenting complaint | treatment | outcome | revision plastic surgery |
|---|---|---|---|---|---|---|
| 1 | 70 | F | pain and erythema on left cheek | Flucloxacillin followed by topical Fucidin cream and Rozex cream | minimally reduced the size of the lesion | surgical removal of her lower left last standing molar, debridement of the intraoral infection and associated cutaneous sinus |
| 2 | 87 | F | Right mandible, right molar tooth | right sided submandibulectomy | raised erythematous plaque, which was tethered to the underlying mandible, and a problematic right molar tooth | extraction of the lower right 5 and biopsy of skin lesion |
| 3 | 12 | M | non healing wound in the right submandibular area | topical antibiotic ointment and a surgical excision | non healing area, 1cm in diameter, located in the submandibular region on the right side | dental extraction of the LR6 and a punch biopsy of the lesion |
| 4 | 38 | M | purulent discharge from a non-healing wound on the right cheek | oral and topical antibiotics | discomfort and pain on biting over the right mandibular teeth. the last standing right lower molar was unresponsive to hot and cold stimuli | The tooth was extracted. Curettage of granulation tissue was conducted. the sinus lining was partially removed from the extraoral area and a biopsy of the skin lesion was taken. |
| 5 | 82 | F | recurrent infections of a fistula at the junction of the submental and right submandibular region | oral and topical antibiotics. excision of the skin lesion was attempted twice. | no cure of the problem and leaving the patient with scar of 2cm | surgical removal of LR 5 |
Case 1:
A 70-year old patient was referred to the Dermatology department by her general practitioner (GP) because of a non-healing lesion on her left cheek. She reported that the skin problem originally started in November 2012 when she developed pain and erythema in her left cheek and neck almost overnight. Originally, her symptoms were diagnosed as cellulitis and responded to a course of oral Flucloxacillin. The lesion then subsequently flared up and a biopsy was taken by the GP due to concern it might be a squamous cell carcinoma. The patient had a further two courses of oral Flucloxacillin followed by topical Fucidin cream (Fusidic acid) and Rozex cream (Metronidazol), which both minimally reduced the size of the lesion. On examination, she had an indurated, tethered lesion on the left lower cheek measuring 2cm x 1cm (Figure 1a). This lesion was surrounded by firm tissue, with a red- brown discolouration and there was no evidence of lymphadenopathy. As the patient demonstrated carious teeth, she was referred to the Craniofacial Department for further management. An OPG and CT scan were ordered for further imaging which demonstrated an intact cortex of the mandibular ramus. However, it was noted that superior to the skin lesion, there was a smooth defect in the superficial cortex of the bone around the tip of the root of the last standing molar (Figure 1b). We performed a surgical removal of her lower left last standing molar, debridement of the intraoral infection and associated cutaneous sinus. One week postoperatively, on review, the area has settled considerably. Intraoral, the mucosa has healed well with no evidence of discharge or tenderness on palpation and the cutaneous surface had re-epithelialised.
Figure 1(a-c).Skin lesion pre-operatively, Computed Tomography scan pre-operatively and scar post-operatively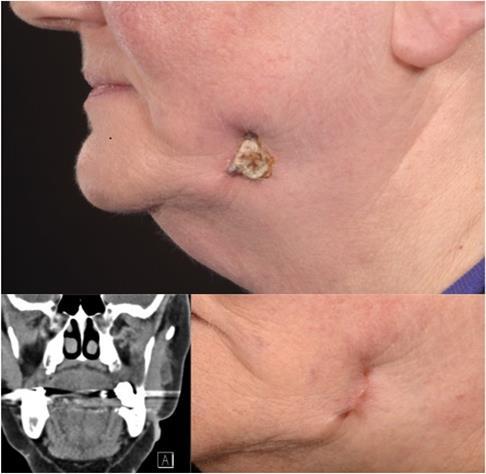
The microbiology results showed only typical oral and cutaneous super-infection with no evidence of any acid-fast bacilli or actinomyces involvement. The histology showed partly ulcerated skin with granulation tissue and acute on chronic inflammation, haemosiderin laden macrophages and foreign body type giant cells. No evidence of dysplasia or malignancy was seen.
11 months post operatively, the patient’s lesion had fully healed and she was very pleased with the aesthetic result. (Figure 1c).
Case 2:
This case was an 87-year-old Caucasian lady was also referred to the ENT department for a right sided submandibulectomy by her local Otolaryngologist. On examination, there was a 1cm raised erythematous plaque, which was tethered to the underlying mandible. Intraoral examination revealed a problematic right molar tooth (Figure 2a-c). On suspicion of an infected dental sinus as the cause of her symptoms, an OPG was performed and the patient was referred to the craniofacial unit afterwards. We performed an extraction of the lower right 5 and biopsied the skin lesion. The microbiology results were similar to those found in Case 1, demonstrating typical oral and cutaneous super-infection with no evidence of any acid-fast bacilli or actinomyces involvement. The histology findings were the same as in the first case.
Shortly after the procedure the skin wound started to heal and 6 months post treatment the patient reported no problems in this area.
Figure 2a-c.Skin lesion right submental region and intra-oral examination finding
Case 3
This was a referral made to the ENT department by a GP of a 12-year-old school boy who had a non healing wound in the right submandibular area. His GP and another ENT-Department had previously treated him for several months with topical antibiotic ointment and a surgical excision was also performed, however, the non healing area recurred shortly after the procedure.
On clinical examination, the lesion was 1cm in diameter and was located in the submandibular region on the right side. A 2.5 cm scar after attempted excision of the skin lesion was noted. A thorough history revealed, from the patient and his parents, multiple dental problems and treatments in the past (Figure 3 a-b). The patient was then referred to our department.
Figure 3a-c.Skin lesion right submental area, OPG mixed dentition with moderately restored LR6 and UR6, a big cavity around the LL6 and periapical radiolucany around LR6
The performed OPG showed a mixed dentition with moderately restored LR6 and UR6, a big cavity around the LL6 and periapical radiolucany around LR6 (Figure 3c). We performed a dental extraction of the LR6 and a punch biopsy of the lesion. The microbiological and histological results were similar to the first two cases described and shortly after the procedure the wound healed well with no recurring problems or lesions reported.
Case 4
This case was referred from the dermatologists and was a 38-year-old male complaining of a purulent discharge from a non-healing wound on the right cheek (Figure 4). The patient thought the lesion was due to his shaving technique, but noted no improvement after changing to an electric razor from a hand held razor. The patient was prescribed oral and topical antibiotics by the GP, but no improvement was observed. On examination by our dermatology colleagues a carious last standing lower right molar was seen and the patient was then subsequently referred to our clinic. The patient reported that he had experienced discomfort and pain on biting over the right mandibular teeth 4 months earlier. Upon further examination, the last standing right lower molar was unresponsive to hot and cold stimuli. The tooth was subsequently extracted, revealing a vertical root fracture. Curettage of granulation tissue was conducted in the socket, and bone resorption at the lingual side of the tooth was confirmed. Finally, the sinus lining was partially removed from the extraoral area and a biopsy was taken out of the skin lesion. Pathological analysis confirmed that the tract was lined with granulation tissue without any epithelial tissue. 5 months after this treatment the cutaneous sinus tract had completely healed with minimal scarring.
Figure 4.Non-healing wound on the right cheek
Case 5:
This 82-year-old women was referred to the department for otolaryngology due o recurrent infections of a fistula at the junction of the submental and right submandibular region. The patient had had these symptoms for several years. She was fit and well medically and the referring practitioner asked for a submandibulectomy to cure the chronic infection. The patient was prescribed oral and topical antibiotics by the GP, but no improvement was observed. An attempted excision of the skin lesion was performed twice in the last 3 years with no cure of the problem but leaving the patient with scar of 2cm. The patient was wearing total dentures and all teeth were surgically removed years previously. However, the performed OPG showed a leftover root of the LR 5. After surgical removal of the tooth the chronic fistula regressed in the following weeks. (Figure 5).
Figure 5.Chronic infection and fistula on the right submental/submandibular side
Discussion
Differential diagnosis of a cutaneous sinus tract should include supportive apical periodontitis, osteomyelitis, pyogenic granulomas, congenital fistulae, salivary gland fistulae, infected cysts and deep mycotic infection. Skin lesions such as pustules, furuncles, foreign-body lesions, squamous cell carcinoma, basal cell face carcinomas and granulomatous disorders may appear superficially similar to a draining sinus tract of dental origin, but they are not true sinus tracts 7, 10. Nearly 80% of reported cases of odontogenic cutaneous sinus tracts have been associated with mandibular teeth infections and 20% with maxillary teeth infections. The cutaneous fistula itself is located in gaps of the mimic muscles of the face, in the area of the platysma, submandibular and submental area as well as the neck. 2, 3, 6, 14, 16.
The evaluation of a cutaneous sinus tract must begin with a thorough history and an awareness that any cutaneous lesion of the face and neck could be of dental origin is absolutely essential. As shown in our cases, the appearance of the skin lesion can be diverse. Unfortunately, in many cases, emphasis is placed only on the skin changes seen and thus the poor dental status of the patient is often overlooked. In all of our reported cases, the initial investigation and treatment by the local GP or ENT doctor was antibiotic therapy and in two of our reported cases, surgical treatment was performed, without success. If no improvement occurs after this treatment, it is essential that a thorough dental examination is performed by the treating doctor, a dentist or a maxillofacial surgeon. Pulp tests and periradicular diagnostic testing should be performed on the suspected tooth and adjacent teeth. More than 1 tooth may be pulpally involved and associated with the cutaneous odontogenic sinus tract. A complicating factor that should be taken into consideration is that the skin lesion does not always directly correspond to the damaged or infected tooth. In addition, the causative tooth might be completely asymptomatic and thus the diagnosis will seem even more unlikely to the inexperienced eye 1, 2, 3, 7, 8, 9, 11, 17.
We performed an OPG in all of our cases, after which no further imaging was needed. Shobatake et al. reported in 2014 that the use of ultrasound is also very effective in the diagnosis of a cutaneous sinus tracts of dental origin 18. Usually, a computed tomography scan or ConeBeam is not necessary however, 2 of the patients documented in this paper had already received a CT scan prior to their referral to our department.
Definitive treatment of the draining sinus tract requires elimination of the source of infection. We performed surgical removal of the infected tooth, debridement of the intraoral infection and associated cutaneous sinus tract in all the 5 reported cases. All patients were free of symptoms after this therapy and there were no reports of recurrence. There is a general agreement in the literature that the infected tooth needs to be treated as a cause of the problem. This can be done with nonsurgical endodontic therapy, root canal therapy, in case of restorable tooth, or by extraction in case of non-restorable tooth. Some studies have recommended complete excision of the sinus tract lining 2, whereas others have contended that surgical treatment and antibiotic therapy are not necessary following dental treatment 6, 8, 10, 17, 19.
Systemic antibiotic administration is not recommended in patients with a cutaneous odontogenic sinus tract who have a competent immune system and no signs and symptoms of systemic involvement. The only patient in our series that received antibiotics was case 5, as he had recurrent abscesses in the operated area and thus was covered postoperatively. All other cases were not administered antibiotics and showed no signs of infection after surgical removal of the tooth causing the dental sinus problem.
A wide external surgical exposure of the sinus tract is not necessary as this leads to unnecessary scarring, a significantly prolonged operation time which makes general anaesthesia more likely and can subsequently lead to iatrogenic injury to mandibular nerve.
Cosmetic surgical treatment may be required at a later date if the healing results in cutaneous retraction or dimpling. In these cases, we perform a surgical scar revision and also, if necessary, use Coleman fat-transfer.
The majority of cases reported in literature regarding dental sinus tract infections are in adult patients but as shown in our case series, or as in a case series published by M. Gupta, these infections can also occur in children and thus the diagnosis in children must not be overlooked 2
Early diagnosis and prompt treatment minimise patient discomfort and aesthetic problems, reducing the possibility of further complications, such as sepsis and osteomyelitis.
Conclusion
Cutaneous facial sinus tracts of odontogenic origin are often initially misdiagnosed despite adequate documentation in the literature. This leads to prolonged and inappropriate treatment. Correct diagnosis and treatment will result in predictable and rapid healing of these lesions and thus it is essential to record case series of dental sinus tracts, to ensure that medical professionals are aware of the presenting symptoms- which can often be very subtle and in the absence of dental pain. In our opinion, based on the findings from our case series, removal of the carious tooth, including the infected pulp canal tissue without laying open the fistula from the outside, is the required treatment for carious teeth.
Ethics
This retrospective review was undertaken with the verbal and written consent of each patient for their case to be published. High ethical standards including data protection were adhered to throughout.
Acknowledgements
Medical Illustration Department, Chelsea and Westminster Hospital, London.
References
- 1.Abuabara A, Schramm C A, Zielak J C, Baratto-Filho F. (2012) Dental infection simulating skin lesion. An Bras Dermatol. 87(4), 619-21.
- 2.Gupta M, Das D, Kapur R, Sibal N. (2011) A clinical predicament--diagnosis and differential diagnosis of cutaneous facial sinus tracts of dental origin: a series of case reports. Oral Surg Oral Med Oral Pathol Oral Radiol Endod;. 112(6), 132-6.
- 3.Herd M K, Aldridge T, Colbert S D, Brennan P A. (2012) Odontogenic skin sinus: a commonly overlooked skin presentation. , J Plast Reconstr Aesthet Surg; 65(12), 1729-30.
- 5.Kumar U, Dharmani C K, George B J, Abraham S.Conservative management of persistent facial cutaneous sinus tract with a dental origin. BMJ Case Rep. 2014-2014.
- 6.Mittal N, Gupta P. (2004) Management of extra oral sinus cases: a clinical dilemma. , J Endod; 30(7), 541-7.
- 7.Pasternak-Junior B, Teixeira C S, Silva-Sousa Y T, Sousa-Neto M D. (2009) Diagnosis and treatment of odontogenic cutaneous sinus tracts of endodontic origin: three case studies. , Int Endod J; 42(3), 271-6.
- 8.Yadav S, Malik S, Mittal H C, Puri P. (2014) Odontogenic cutaneous draining sinus. , J Craniofac surg; 25(1), 86-8.
- 9.Bai J, Ji A P, Huang M W. (2014) Submental cutaneous sinus tract of mandibular second molar origin: a case report. , Int Endod J; 47(12), 1185-91.
- 10.Johnson B R, Remeikis N A, Van Cura JE. (1999) Diagnosis and treatment of cutaneous facial sinus tracts of dental origin. , J Am Dent Assoc; 130(6), 832-6.
- 12.Pedrazzetti P, Harms M. (2000) [What is your diagnosis? Mandibular dental fistula. Syn: dentogenic fistula, cutaneous dental sinus]. , Praxis; 89(44), 1775-8.
- 13.Tan K W. (2014) Images in clinical medicine. Discharging dental sinus tract. , N Engl J Med; 371(9), 846.
- 14.Witherow H, Washan P, Blenkinsopp P. (2003) Midline odontogenic infections: a continuing diagnostic problem. , Br J Plast Surg; 56(2), 173-5.
- 16.Tidwell E, Jenkins J D, Ellis C D, Hutson B, Cederberg R A. (1997) Cutaneous odontogenic sinus tract to the chin: a case report. , Int Endod J; 30(5), 352-5.
- 17.Holt R, Roberts G, Scully C. (2000) ABC of oral health. Oral health and disease. , BMJ; 320(7250), 1652-5.
Cited by (2)
This article has been cited by 2 scholarly works according to:
Citing Articles:
International Journal of Clinical Pediatric Dentistry (2022) Crossref
International Journal of Clinical Pediatric Dentistry (2022) OpenAlex