
Abstract
Objectives
Our study aims to determine the trend of the antibody titer and assess the efficacy of the vaccine.
Methods
It was conducted on 983 healthcare professionals between 27 February 2020 and 22 October 2021 at the Local Health Authority (ASL) of Rieti. Workers voluntarily underwent serological testing before vaccination (T1), at least 15 days after vaccination (T2), and at least 150 days after vaccination (T3). We picked individuals who had received two doses of the vaccine. As for positivity, we assessed incidence – and therefore symptomatology – in three time intervals. We used a contingency tables for the analysis and tested the relation to the chi-square test and ANOVA test. Regarding differentials in terms of antibody capacity, we considered different time intervals: the methodological approach was the same.
Results
The average value of the dimeric serological testing at T1 was equal to 28.80 AU/mL, which increased to 220.55 AU/mL at T2, and then decreased to 143.62 AU/mL at T3 (P = 0.000). At T2, the number of people with a protective titer was equal to 95.96% of the total; at T3, it was equal to 96.39% (P = 0.019). Before the vaccination campaign, 75 workers tested positive (25 paucisymptoms, 4 severe symptoms). After vaccination, 14 workers tested positive: almost all were asymptomatic.
Conclusion
Vaccination determines a statistically significant variation of the average value of antibody titer, a statistically significant reduction of positive swab tests and a better prognosis.
Author Contributions
Academic Editor: Lucio Mango, Health management" University Master, University of International Studies (UNINT) – Rome, Italy, Chief Nuclear Medicine Unit, “S. Camillo-Forlanini” General Hospital – Rome, Italy.
Checked for plagiarism: Yes
Review by: Single-blind
Copyright © 2022 De Luca A, et al.
 This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Competing interests
The authors have declared that no competing interests exist.
Citation:
Introduction
The study of the seroconversion of individuals with a positive history of SARS-CoV-2 infection offers important considerations: relevant literature shows us different results, especially for the duration of the antibody titer. Seroprevalence studies were carried out in the pre-vaccination period to identify the immunization status of the working population and any possible asymptomatic carriers.
A study 1 carried out in England by Cooke et al. three months after the peak of the first wave shows an overall 6% seroprevalence (95% CI: 5.8-6.1), with higher antibody titers in high density urban centres. 4.5 and 6 months after the peak of the first wave there was a 19% (95% CI: 16.1-21.8) and 26.5% (95% CI: 23.8-29.0) reduction.
Differently, the study 2 carried out in Vo' Euganeo by the University of Padua, led by Professor Crisanti, shows us different results. In 98.8% of cases (CI: 93.7-100.0%), individuals who underwent serological testing in May 2020 were still reactive to at least one antigen when they were tested again in November 2020, with an increase in antibody titer or in neutralising antibodies in 18.6% of cases (CI: 11.0-28.5%).
As for seroconversion in vaccinated individuals, short-term seroprevalence studies have been carried out to assess the efficacy of the vaccine, as well as its ability to reduce infection rates and improve the prognosis.
Mark G. Thompson et al. carried out a prospective study 3 on 3,975 healthcare workers in the United States of America aimed at detecting SARS-CoV-2 through nasal swabs: the test came back positive in 204 participants (5%), 5 of whom were fully vaccinated, 11 were partially vaccinated, and 156 were not vaccinated. The efficacy of the vaccine was rated at 91% in fully vaccinated individuals, and 81% in partially vaccinated individuals. The risk of feverish symptoms was 58% lower (relative risk, 0.42; 95% CI, from 0.18 to 0.98) and the duration of the disease was shorter, with 2.3 fewer bed rest days.
Similar results are seen in the study 4 carried out by Chung et al. in Canada, which shows that two doses of the mRNA vaccine are highly effective against symptomatic infections and for prognostic purposes, thus reducing the risk of severe outcomes. In detail, the efficacy of the vaccine after an interval greater than or equal to 14 days after the first dose was rated at 60%, rising to 91% at an interval greater than or equal to 7 days after the second dose. Efficacy against hospitalization or death was rated at 70% after an interval greater than or equal to 14 days after the first dose, and 98% after an interval greater than or equal to 7 days after the second dose.
Our study has two main objectives: the first is to assess the seroprevalence of antibodies against the infectious agent SARS-CoV-2 following vaccination among healthcare workers at the ASL of Rieti.
The second is to evaluate the efficacy of the vaccine in terms of reducing SARS-CoV-2 infectivity and virulence, thus improving the prognosis for infected patients.
Experimental Procedure
We picked individuals who had received two doses of the vaccine. As for positivity, we assessed incidence – and therefore symptomatology – in three time intervals: before the first dose, between the first and the second dose, and after the second dose. We used a contingency table for the analysis and tested the relation to the chi-square test. Regarding differentials in terms of antibody capacity, we considered different time intervals. The methodological approach was the same, with the difference that in this case the antibody titer (measured with both dimeric and trimeric tests) is a metric variable and therefore the calculations were based on an analysis of the inter-period variation (and with an intra-period look based on intra-period standard deviations). Moreover, ANOVA (analysis of variance) was used for the analyses on dimeric and trimeric measurements, with the addition of the eta-squared coefficient (eta-squared is a normalized index: it takes a value of 0 when all conditional means are the same, in which case we talk about independence). Regarding the distribution of positive workers by time interval and role (and symptomatology by time period), we once again used the contingency table, which is supported by using the chi-square test. Lastly, to assess coherence among the results of dimeric and trimeric measurements, we used the Pearson correlation coefficient.
Materials and Methods
Seroprevalence surveys were carried out at the ASL of Rieti even before the start of the vaccination campaign, with the aim of studying the immunization status of the working population, supporting the survey with the periodic testing of nasal swabs for the early identification of any possible asymptomatic carriers, so as to stop new outbreaks early on.
The first seroprevalence campaign with the determination of serum IgG levels was carried out at the ASL of Rieti between 4 May 2020 and 31 July 2020, and then again between 15 September 2020 and 29 January 2021.
After identifying a person in charge who would be responsible for blood sampling and obtaining informed consent, testing was carried out in the blood drawing rooms in the various centres of the ASL or in the workers’ hospital wards.
The dimeric LIAISON® SARS-CoV-2 S1/S2 IgG test was used in both above-mentioned campaigns to determine the antibody titer.
All those who tested positive for IgG with no previous history of SARS-CoV-2 infection underwent a nasopharyngeal swab test to detect the virus.
In addition, since December 2020, workers at the ASL of Rieti have been periodically subject to rapid antigen testing. In case of a positive outcome, a molecular nasopharyngeal swab was and is performed to confirm the result.
The vaccination campaign against COVID-19 for healthcare workers was launched at the ASL of Rieti starting on 27 December 2020.
Following the recommendations made by the Ministry of Health, healthcare workers were vaccinated as a priority category. First, priority was given to those with a negative recent and remote medical history of SARS-CoV-2, while those who had already been infected were vaccinated later on.
The COVID-19 Comirnaty (Pfizer) vaccine was used.
Following vaccination, a seroprevalence survey was conducted to verify the antibody response.
Starting on 12 February 2021, workers at the ASL of Rieti who had completed the vaccination cycle were invited to give a blood sample at least 15 days after the second dose to verify the antibody titer.
The LIAISON® SARS-CoV-2 TrimericS IgG test and the LIAISON® SARS-CoV-2 S1/S2 IgG test were introduced to determine the antibody titer in this phase of campaign (view supplementary material).
Informed consent was collected from the coordinator/person in charge for each worker who underwent blood sampling to determine antibody titers as part of the seroprevalence survey. Results were kept by the coordinators/persons in charge.
The dimeric test was the first to be made available on the market and has fewer recognition epitopes on the spike protein antigen. The trimeric test was made available on the market later on and is more sensitive as it recognizes the entire spike protein antigen three-dimensionally.
In the time interval between 22 September 2021 and 22 October 2021, all workers were given the chance to take part in screening through a venous blood sample for the search of antibodies against SARS-CoV-2 and, once again, the dimeric and trimeric swab tests were used.
All workers who underwent at least three observations for the serological testing were included in this study.
The following individuals were excluded from our study:
1. Individuals who did not undergo at least 3 observations.
2. Individuals who did not complete the vaccination cycle following the variable protocols based on the case.
3. Individuals who did not receive vaccination.
4. Individuals who received vaccination after the start of the campaign, forcing us to carry out the third observation at T3 at a time interval less than 150 days after completing the vaccination cycle.
The first observation was carried out before the vaccination campaign, at least once in the two above-mentioned periods that go from 4 May 2020 until 31 July 2020, and from 15 September 2020 until 29 January 2021. Only one observation was considered for each worker – when available, the most recent observation or the following one. Hereinafter, this first time interval referring to all tests performed before the vaccination campaign will be labelled as “T1”. For this first observation at T1, only the dimeric test is available.
The second observation was carried out after completing the vaccination cycle, following the protocol for the time interval considered, at least 15 days after vaccination. Hereinafter, this second time interval, referring to the time after completing the vaccination cycle, will be labelled as “T2”. For the second observation at T2, both the dimeric and trimeric tests were used. The average time distance between the second dose of the vaccine and the blood test at T2 is equal to 43.8 days, with a minimum value of 16 days and a maximum value of 64 days. All blood tests at T2 were performed between 12 February 2021 and 30 May 2021.
The third observation was carried out at least 150 days after completing the vaccination cycle, between 22 September 2021 and 22 October 2021. Hereinafter, this third time interval will be labelled as “T3”. Once again, as for the previous observation, both tests were used. The average time distance between the second dose of the vaccine and the blood test at T3 is equal to 183.4 days, with a minimum value of 159 days and a maximum value of 203 days.
Workers also underwent molecular and antigen swab tests. These tests were performed at our health facility as routine screening which started in December 2020, in case of close contact with a positive SARS-CoV-2 patient, or in case of COVID-like symptoms.
Data were collected by gender, age, role, whether and when one had a positive result from the rapid nasal antigen swab test or molecular nasopharyngeal swab test, the severity of the disease and clinical course in case of a positive swab test, and when the COVID-19 vaccine was administered.
For these reasons, it should be emphasized that the population under study was not randomly drawn from the total population, but this population constitutes a sample of subjects selected on the basis of logical criteria related to the working hypotheses (as just described above). The parameters of the sampled population studied (gender and age distribution) are very similar to those of the total population working in the Local Healthcare firm examined in this study.
The sample of healthcare workers for the present study was selected based on the above-mentioned criteria: 983 workers at the ASL of Rieti, with an average age of 47.53 years, 73.90% of whom were women and the rest were men (Table 1). The total population of the health institution studied amounted to 2285 workers (71.6 women and 28.4 men), with a mean age of 47.12 (with a standard deviation of 11.02 years). Comparing the distributions by occupational duties of the sample in the total population and the sample studied, there are no differences greater than 2% for each category. In this sense, the two populations are largely overlapping.
This made it possible to assess the vaccination status of individuals with a negative swab test, as well as the clinical course of the disease.
The course of the disease was divided into four clinical pictures:
1. Asymptomatic: when workers show no symptoms.
2. Paucisymptomatic: when workers present with mild symptoms.
3. Symptomatic: when workers present with the typical symptoms of the disease – i.e. fever, cough, dyspnoea, ageusia, anosmia, bowel changes – but can be cured at home and do not require hospitalization.
4. Severe Symptoms: when workers present with severe symptoms and require hospitalization.
Table 1. Description of the study population (Rieti, Italy. 2020-2021)| N | (%) | Age (m ± s) | min | max | |
| Total | 983 | (100) | 47.53 ± 10,245 | 22 | 68 |
| Gender | |||||
| Female | 726 | (73.90) | 47.55 ± 10,026 | 23 | 68 |
| Male | 257 | (26.10) | 47.48 ± 10,861 | 22 | 68 |
Results
We tested the incidence of positive swab tests in our population, from the beginning of the pandemic until the end of our study on 22 October 2021. 127 workers had a positive molecular or antigen swab test, out of a total population of 983 workers (12.92%). Following participation in the vaccination campaign, the number of positive swab tests among healthcare workers seems to change: 75 healthcare workers tested positive before receiving the vaccine, 38 after the first dose, and only 14 after completing the vaccination cycle. The overall variation in the time interval considered is statistically significant with the chi-square test for P = 0.005 (Graph 1).
The trend of the severity of the disease was assessed in healthcare workers with a positive swab test for no dose, after first dose, after second dose period. The overall variation of the entity of symptomatology in the time interval considered is statistically significant with the chi-square test for P = 0.05 (Graph 2).
Graph 1.Number of workers with positive swab tests, related to the vaccination status (Rieti, Italy. 2020-2021). Chi-square test significant for P = 0.005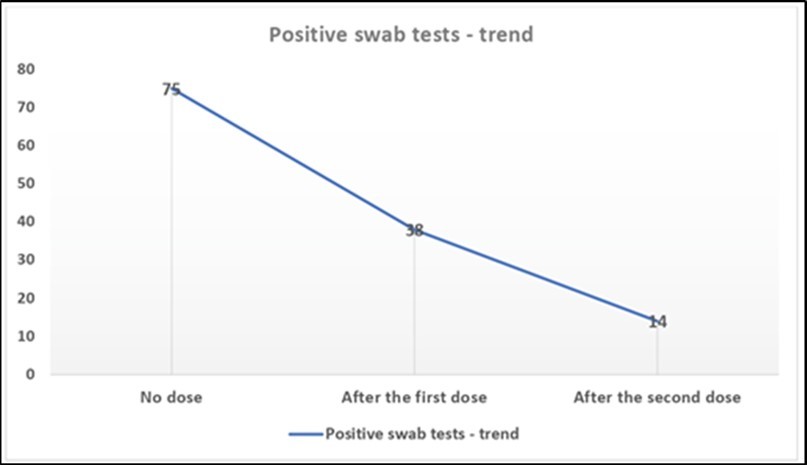
Graph 2.Distribution of the entity of symptomatology in positive workers, related to vaccination (Rieti, Italy. 2020-2021).
We analysed the distribution of healthcare workers by professional profile with a positive swab test in the three time intervals considered (Table 2). When no healthcare workers were vaccinated, there was a higher incidence of positive swab tests in the nursing sector with 61.3% of the total, followed by 20% physicians, and 5.3% personal care workers, healthcare professionals and assistants. Even analysing the distribution of positive swab tests of workers who had already received the first dose of the vaccine, we notice figures remain similar. The overall variation reported in Table 2 in the time interval considered is statistically significant with the chi-square test for P = 0.0000.
Table 2. Positivity by professional profile and role (Rieti, Italy. 2020-2021)| Before the vaccination campaign | Between the first and the second dose | After the second dose | ||||
| N | (%) | N | (%) | N | (%) | |
| Other technical personnel | 0 | (0.0) | 0 | (0.0) | 0 | (0.0) |
| Social workers | 0 | (0.0) | 0 | (0.0) | 0 | (0.0) |
| Healthcare managers | 0 | (0.0) | 0 | (0.0) | 0 | (0.0) |
| Administrative personnel | 2 | (2.7) | 1 | (2.6) | 0 | (0.0) |
| Nurses | 46 | (61.3) | 24 | (63.2) | 9 | (64.3) |
| Physicians | 15 | (20.0) | 8 | (21.1) | 1 | (7.1) |
| Personal care workers / Healthcare professional / Assistants | 4 | (5.3) | 3 | (7.9) | 2 | (14.3) |
| Technician for prevention of environment and in the workplace (TDP) | 2 | (2.7) | 0 | (0.0) | 0 | (0.0) |
| Healthcare technician | 1 | (1.3) | 0 | (0.0) | 0 | (0.0) |
| Therapists | 5 | (6.7) | 2 | (5.3) | 2 | (14.3) |
| Total | 75 | (100.0) | 38 | (100.0) | 14 | (100.0) |
The following analyses were carried out on 943 workers and not on the total 983 of our sample population. In fact, to limit heterogeneity and make sure the sample population were as homogeneous as possible in the variable considered in the three time intervals, we excluded 28 workers at T2 who had only received one dose of the vaccine due to positive history of SARS-CoV-2 infection, and 14 workers who were infected with COVID-19 after completing the vaccination cycle.
Table 3 shows that even before the vaccination campaign, 18.17% of our sample population had a reactive dimeric serological testing. At T2, the number of workers who developed a protective antibody titer was 95.86%, remaining more or less stable at T3 (95.96%) (Chi-square test significant for P = 0.009).
Table 3. Outcome of the dimeric test in workers in the different time intervals (Rieti, Italy. 2020-2021)| Reference values | T1 | T2 | T3 | |||
| N | (%) | N | (%) | N | (%) | |
| < 11.9 – Non-reactive | 764 | (81.19) | 37 | (3.93) | 35 | (3.72) |
| > 12 e <14.9 – Uncertain value | 6 | (0.64) | 2 | (0.21) | 3 | (0.32) |
| >15 – Reactive | 171 | (18.17) | 902 | (95.86) | 903 | (95.96) |
| Total | 941 | (100) | 941 | (100) | 941 | (100) |
The average value of antibodies against SARS-CoV-2 on the venous blood sample was analysed with the LIAISON® SARS-CoV-2 S1/S2 IgG test in the three time intervals considered (Table 4). At T1, the average value was 28.80 AU/mL due to the number of positive cases before the start of the vaccination campaign. At T2, the average value settled at 220.55 AU/mL. Such value can be considered protective as it is over the cut-off set at 15 AU/mL for this method. This figure decreases to 143.62 AU/mL at T3 (ANOVA significant for P = 0.000; Eta-squared = 0.549 significant for 0.000).
In Table 4, the average IgG value with the trimeric test at T2 is equal to 1,792.81, and decreases to 1,402.54 at T3, remaining well-over the cut-off value for this test; the variation between the two time intervals is statistically significant (ANOVA significant for P =0.000, Eta-squared = 0.576 significant for 0.000).
Regarding the number of healthcare workers with a protective titer with a trimeric test, the variation between T2 – where 95.96 % are protected – and T3 – where 96.39% are protected – is not statistically significant (Chi-square test significant for P = 0.019 - > the differences in the values by period are not significant).
Table 4. Average value time trend – dimeric and trimeric tests (Rieti, Italy. 2020-2021)| eriod | Dimeric Test Value (m ± s) | Trimeric Test Value (m ± s) |
| T1 | 28.8029 ± 84.16049* | - |
| T2 | 220.5479 ± 114.2066* | 1,792,814 ± 4,714,409** |
| T3 | 143.6246 ± 102.5477* | 1,402,536 ± 4,484,841** |
Correlations were assessed for the two time intervals for which data is available for the same cases (observations) based on the measures of dimeric and trimeric tests. The result is relevant since the correlation coefficient shows a level of overlap and coherence between the two texts. In the first of the two double measurement periods, the correlation coefficient is equal to +0.95 (with full significance, with a P-value of 0.000); in the second time interval of double measurement, such coefficient is equal to +0.97 (with full significance, with a P-value of 0.000). This overlap is fully consistent with the evidence relating to the cut-off levels by time period of the two tests.
Discussion
The results show the efficacy of the vaccine in determining both a reduction of infectivity – in the strictest sense of the term, i.e., the ability of a microorganism to colonize a host receptor – and virulence – i.e., the ability of the virion to determine pathological conditions after colonizing the host.
Graph 1 presents the positivity rates analysed and shows the frequency of the event "Positive Outcome" following a molecular or antigen swab test, carried out for screening or in those healthcare workers who may have come in contact with the virus.
It is clear that there is a decreasing trend among vaccinated workers.
There is a statistically significant variation of the incidence of positive swab tests following the start of the vaccination campaign, going from 75 healthcare workers among our sample population with a positive swab test before vaccination, to 14 after completing the vaccination cycle.
In line with the other studies mentioned above, it is interesting to see that the vaccine is not only effective in reducing infectivity, but also the virulence of SARS-CoV-2. Focusing on Graph 2, in particular on the first two columns on the distribution of the severity of symptoms at the first time interval – i.e., before the vaccine – and the second time interval – i.e., after the first dose.
The efficacy of a single dose of the vaccine is clear; it reduces symptoms and improves the prognosis. In fact, there is an increase in the number of paucisymptomatic patients (from 41.32% to 47.37%), and a decrease in symptomatic patients (from 33.32% to 28.95%) and those who require hospitalization (from 5.32% to 5.26%.)
The second dose of the vaccine ensures an even better prognosis; only 14 fully vaccinated workers tested positive and, of these, more than half (78.58%) presented with a paucisymptomatic or asymptomatic infection. Only 2 workers became symptomatic, and no one developed severe symptoms that required hospitalization.
These results are certainly encouraging and allow us to assert that the vaccine has protected our population as it was proven in Gareth Iacobucci’s study 5 in Israel, where 21 days after the first dose of the AstraZeneca or Pfizer vaccine, the rates of all new SARS-CoV-2 infections decreased by 65%, symptomatic infections by 72%, and asymptomatic infections by 57% (P < 0.001 for all). As for those who received the second dose of the Pfizer vaccine, infections were 70% lower (62% to 77%; P < 0.001), and symptomatic infections were 90% lower (82% to 94%; P < 0.001). In this study the sample size is larger than ours and carried out on the general population, not on health workers as in our case. They did not even detect differences in efficacy based on age, between over and under 75. However they found a greater reduction in symptomatic infections rather than asymptomatic forms, suggesting the possibility of reinfection also after vaccination.
Table 2 shows that within the sample population – i.e., workers at the ASL of Rieti – there is a higher incidence of positive swab tests among the professional profiles more exposed to contact with patients. Before the vaccine, after the first dose, and after the second dose, physicians and nurses account for 81.3%, 84.3%, and 71.4% of the total positive swab tests.
This leads us to different observations. According to recent publications, like the study 6 carried out by Oster et al., the most critical moment for contagion remains the extra-occupational context, even for healthcare workers: longer contact with no social distancing and often lack of personal protective equipment are still the most dangerous risk factors. According to this, one may think that in our specific case, after the first dose of the vaccine, people mistakenly become less cautious outside the workplace. Despite this, the same authors declare that their study is in line with others carried out on the general population. However, they enhance among all the limits of the study, its retrospective character and the small dimension of the sample. To overcome this limit, they select three negative controls for each case and they finally suggest re-evaluating the quarantine for vaccinated operators in the event of a positive cohabitant.
On the other hand, in his article 7 Claudio Beltramello offers different points of view, stressing that healthcare workers are 5 times more exposed to the risk of infection than the general population due to the pace of work and the incorrect use of personal protective equipment.
All this comes with an important final reflection which shows that the greater risk for healthcare workers (5 times higher) could depend on the unhealthy practice of admitting outside patients with an antigen swab test.
This test is burdened by less than 70% sensitivity rate, thus resulting in 1 to 3 negative tests in every 10 people who are actually infected. This is interesting if compared with our framework in which the incidence is higher in workers who are closer to and more in contact with patients. According to the monitoring 8 carried out by the National Institute for Insurance against Accidents at Work (INAIL) and the Italian National Institute of Health (ISS), 15,926 healthcare workers tested positive from the beginning of the pandemic until 30 April 2020.
The same source shows a higher incidence in the 50-59 age group and in the nursing sector with 47.9% of total cases, followed by physicians with 20.5% of cases, and finally personal care workers with 19.7%. The same report also analyses distribution by area of intervention and shows a higher incidence in those who work in the health sector (21.2%) compared to those who work in the COVID area (15.6%).INAIL’s latest report 9 on injuries due to COVID-19 confirms that healthcare workers were the most affected. The results of serological testing show that vaccination determines a statistically significant variation of the antibody titer in the period under observation.
The variation is significant when taking into account the average values at the three time intervals – T1, T2, T3 – with the dimeric test, and at T2 and T3 with the trimeric test.
At T2, the average value of the antibody titer is well over the cut-off with both tests, and it stays like that for at least 150 days, despite the decrease (see Tables 4).
Table 3 shows the coverage rate for our sample population: at T2, 95.86% of workers tested with the dimeric test had developed a protective antibody titer, and 95.96% of those tested with the trimeric test. These results conform to the study10 conducted by Pani et all called RENAISSANCE, in which 2,497 vaccinated healthcare workers showed a very high antibody response: in 98.4% of cases, individuals developed the expected antibodies; out of the total sample only 4 were non-responders, all characterized by a state of immunodepression: unfortunately we were not able to evaluate the state of the immune system of our operators. Similar to our study, the incidence of positive swabs at a distance of four months from vaccination is greatly reduced, only 13 operators, of which only one needs hospitalization.
Despite the reduction in the above-mentioned IgG average value between T2 and T3 with the trimeric test (Table 4), it is interesting to see that when assessing the absolute value of healthcare workers with a protective titer, the variation between T2 and T3 is not statistically significant. Those with a titer over the cut-off level right after vaccination keep it also after 150 days.Based on our observations, the same number of healthcare workers who develop an antibody titer immediately after vaccination, also keep it up to at least 150 days, and therefore there should be no time frame when one is uncovered by circulating antibodies.
Conclusion
The statistically significant variations reported in the reduction of positive swab tests and the severity of the disease seem to show the vaccine has a protective effect. We can say that those who develop a protective titer at least 15 days after the vaccination, keep what is considered a protective titer up to at least 150 days after vaccination, even if the protection tends to decrease.With this being said, when our healthcare workers are vaccinated and develop an increase in the antibody titer, there is a statistically significant decrease in positive swab tests.
Regarding this study’s critical issues, the first is definitely linked to the retrospective nature of the study which did not allow us to study all the parameters we would have liked to assess
A first example is the fact that we were not able to assess whether the positive swab tests in vaccinated workers were linked to SARS-CoV-2 variants. This would have been interesting especially if contextualized in the current situation in which several studies, including the one 11 carried out by Keehner et al., have highlighted the loss of efficacy of the vaccine and some variants’ ability to reinfect individuals even when a large part of the population is vaccinated. Such study highlighted an important loss of efficacy of the vaccine, dropping from 90% between March and June, to 65.5% in July.
Another limitation to the study is that of only having a sample of healthcare workers who had received the mRNA Comirnaty (Pfizer) vaccine. It would have been interesting to study whether these results are in line with or opposite from the viral vector vaccines, both in terms of seroprevalence and reducing SARS-CoV-2 infectivity and virulence, or comparing the two mRNA vaccines available, as in the study 12 carried out by Pilishvili et. all in the United States of America. After two doses of the vaccine, such studies showed 89% efficacy for Comirnaty (Pfizer), and 96% efficacy for Spikevax (Moderna).
This takes us to another critical issue, i.e. the composition of our sample population which reduces the value of our study. In fact, the sample population (983 workers) represents 43.02% of the 2,285 total healthcare workers of the ASL of Rieti, numerically reduced compared to that of the province of Rieti (about 152,000 residents). The study population is mainly made of the elderly, as seen in the results, and only of healthcare and personal care workers, therefore individuals who are at a higher risk than the general population. It is clear that this makes our results non-applicable to the rest of the population.
This study is part of the observational research on the population of healthcare workers which was carried out in Italy and at international level during the ongoing COVID-19 pandemic.
The study confirms the importance of a widespread vaccination campaign to prevent the development of SARS-CoV-2 infections. The results are in line with the study RENAISSANCE 10.
The results are also in line with the data on the population of the ASL of Rieti, even though the population of healthcare workers is at a higher risk of infection.
Acknowledgements
We thank Shannon Clay for the English translation. The authors thank all the participants for their cooperation.
References
- 1.W H Cooke, G S Atchison, C M Whitaker, Elliott J, Moshe M et al. (2021) Prevalence of antibody positivity to SARS-CoV-2 following the first peak of infection in England: Serial cross-sectional studies of 365,000 adults. London (UK): Elsevier; The Lancet Regional Health – Europe. 4, 100098.
- 2.Dorigatti I, Lavezzo E, Manuto L, Ciavarella C, Pacenti M et al.Crisanti A.(2021). SARS-CoV-2 antibody dynamics and transmission from community-wide serological testing in the Italian municipality of Vo’. London (UK):. , Nature Publishing Group: Nature Communications 12(1), 4383.
- 3.M G Thompson, J L Burgess, A L Naleway, Tyner H, S K Yoon et al.(2021).Prevention and Attenuation of Covid-19 with the BNT162b2 and mRNA-1273 Vaccines. Boston (USA):Massachusetts Medical Society,New England. , Journal of Medicine 385(4), 320-329.
- 4.Chung H, He S, Nasreen S, Sundaram M E, Buchan S A et al.Effectiveness of BNT162b2 and mRNA-1273 covid-19 vaccines against symptomatic SARS-CoV-2 infection and severe covid-19 outcomes in Ontario, Canada: test negative design study. London (UK): British Medical Journal. 374.
- 5.Iacobucci G. (2021) Covid-19: Infections fell by 65% after first dose of AstraZeneca or Pfizer vaccine, data show. London (UK) British Medical Journal;. 373-1068.
- 6.Oster Y, Benenson S, L Y Harpaz, Buda I, Nir-Paz R et al.Association Between Exposure Characteristics and the Risk for. COVID-19 Infection Among Health Care Workers With and Without BNT162b2 Vaccination.American Medical Association(USA): JAMA Netw Open 4(9), 2125394.
- 7. (2021) Beltramello C.Gli operatori sanitari nella seconda ondata. Saluteinternazionale.it. , (Italy);
- 8.Iavicoli S, Buresti G, Gagliardi D, Petyx M, B M Rondinone et al.Pezzotti P.Monitoraggio sugli operatori sanitari risultati positivi a COVID-19 dall’inizio dell’epidemia fino al 30 aprile 2020: studio retrospettivo in sette regioni italiane. Inail.it; 2021;https://www.inail.it/cs/internet/home.html , Rome (Italy):
- 9.INAIL. (2021) Scheda nazionale infortuni sul lavoro da covid-19. I dati delle denunce al 31 ottobre 2021. , Rome (Italy): Inail.it;
- 10.Cento V, Vismara C, Campisi Di Ruscio F, Romandini A, Senatore M et al. (2021) . Results of the RENAISSANCE Study: REsponse to BNT162b2 COVID-19 vacciNe-short- And long-term Immune reSponSe evAluatioN in health Care workErs. London (UK): National Library of Medicine, Mayo Clin Proc 96(12), 2966-2979.