
Mathematical Modelling of Typhoid Fever Transmission Dynamics and Intervention Impact in Harare, Zimbabwe (2018–2020)
Abstract
Background
Typhoid fever remains a significant public health issue in Harare City, Zimbabwe, exacerbated by recurrent outbreaks between 2018 and 2020. Key challenges, including inadequate water supply and sanitation infrastructure, high population density, and limited healthcare access, have intensified the disease burden. Understanding the key transmission drivers and assessing the impact of various interventions are essential for informing policy and health strategies.
Objectives
This study aimed to: 1: To predict future trends in typhoid fever cases Harare City typhoid hot areas. 2: To develop a mathematical model to simulate the spread of typhoid fever incidence under different intervention scenarios and recommend evidence-based strategies for reducing the disease burden in Harare City.
Methods
A dynamic compartmental SIR-based model, adapted from the Pitzer Vaccine Effectiveness (VE) framework, was employed to simulate disease transmission. This model accounted for both short-cycle (human-to-human) and long-cycle (environmental) transmission pathways. Data from Harare City (2018–2020) were used for model calibration and forecasting, and sensitivity analysis was performed to assess the impact of different intervention levels.
Findings
The model identified inadequate sanitation, contaminated water sources, and low health- seeking behaviors as primary drivers of typhoid transmission. In the absence of interventions, the model projected a sustained high rate of transmission. However, treatment and WASH interventions could reduce the disease burden by 50–60%, while combined strategies incorporating vaccination and education led to an 80% reduction in cases. Sensitivity analysis indicated that treatment and WASH interventions were particularly impactful at moderate coverage levels.
Conclusion
Mathematical modeling effectively demonstrated the multifactorial drivers of typhoid fever transmission in Harare. Integrated interventions that combine WASH, vaccination, treatment, and education present the most promising approach for long-term control of the disease. The findings offer a solid, data-driven foundation for public health decision-making and resource allocation.
Article Information
- Received
- Accepted
- Published
Academic Editor: Mohan Lal, Assistant Professor, Irrigation and Drainage Engineering department, College of Technology, G B Pant University of Agriculture and Technology, Pantnagar, India.
Checked for plagiarism: Yes
Review by: Single-blind
Copyright © 2025 Innocent
 This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Corresponding author: Innocent Mukeredzi, Harare City Health Department, Harare, Zimbabwe —
Competing Interests
The authors declare that the research was conducted in the absence of any commercial or financial retionships that could be construed as a potential conflict of interest.
Funding
No specific funding statement was provided by the authors.
Data Availability
No data-availability statement was provided by the authors.
Acknowledgements
The City Health Department, Harare City
The World Bank, Harare Office
Cordaid, Zimbabwe Country Office
Ministry of Health and Child Care, Zimbabwe
University of Zimbabwe
Author contributions
All authors listed have made a substantial, direct, and intellectual contribution to the work and approved it for publication.
Citation:
Introduction
Typhoid Fever is a significant public health concern in Zimbabwe, particularly in urban areas like Harare City. The disease is caused by Salmonella Typhi and is usually spread through contaminated food and water. Recent data suggest an increasing trend in Typhoid Fever cases in Harare City, highlighting the need for a comprehensive understanding of the drivers of transmission. Typhoid fever is caused by the bacterial pathogen Salmonella enterica serovar Typhi. It is a major cause of illness and mortality in regions with limited access to improved water and sanitation 1. Recent estimates have placed the global burden of typhoid fever at 11.9–26.9 million cases and 129 000–270 000 deaths per year 2.
Although the endemic burden of typhoid fever in South and Southeast Asia has long been recognized, less is known about the burden of disease in sub-Saharan Africa.
In Zimbabwe, as in much of sub-Saharan Africa, nontyphoidal Salmonella (NTS) serovars have been a much more common cause of bloodstream infections over the past 2 decades. Since 2014, however, there has been a substantial increase in the number of confirmed cases of Salmonella Typhi at BRIDH. The number of typhoid cases increased from 64 per year during 2014 -2016 to over 500 cases in 2017. This epidemic of typhoid fever has persisted 3 and coincides with numerous reports of ongoing epidemics of typhoid fever in settings across Africa 4. These epidemics have closely followed the recent global emergence of the H58 haplotype of Salmonella Typhi 5. The H58 lineage is highly clonal and differentiated from other haplotypes using a simple single nucleotide polymorphism–based typing scheme 6, and is associated with high levels of multidrug resistance 5. There are a variety of hypotheses that could explain the large increase in typhoid fever cases in Harare City, including an increase in population density, Inadequate safe water , less hygiene practices, inconsistent vaccination, waning immunity and an increase in the prevalence of multidrug resistant (MDR) strains 7.
Figure 1. Suspected typhoid cases by hospital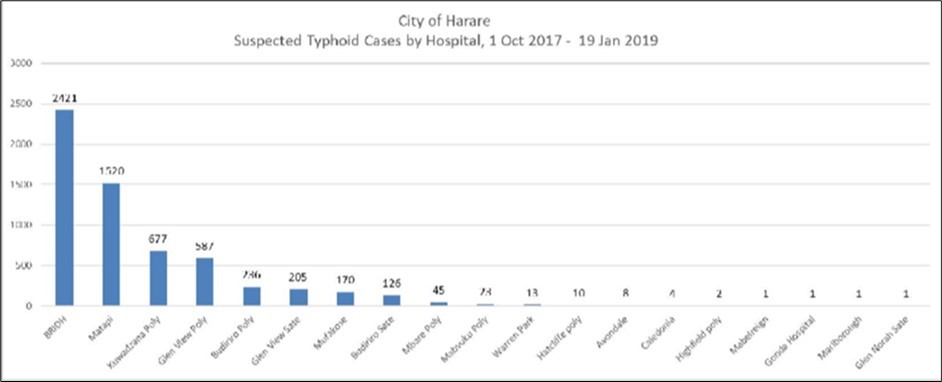
Download figure
The distribution of suspected typhoid cases across various clinics and hospitals in Harare reveals notable disparities in case burden, with a total of 6,051 cases reported. Beatrice Road Infectious Diseases Hospital (BRIDH) recorded the highest number of cases at 2,421, accounting for approximately 40% of the total. This indicates that BRIDH is a central referral point for suspected typhoid cases, likely due to its specialized infectious disease services. Matapi Clinic followed with 1,520 cases (about 25%), suggesting a high burden in Mbare and surrounding high-density suburbs where sanitation challenges are prevalent.
Kuwadzana Polyclinic and Glen View Polyclinic recorded 677 and 587 cases respectively, reflecting significant caseloads likely linked to water and sanitation infrastructure in these suburbs. Budiriro and Glen View Sate clinics also recorded considerable numbers (236 and 205 respectively), further emphasizing the concentration of cases in high-density western suburbs of Harare.
Other facilities such as Mufakose (170 cases) and Budiriro Sate (126 cases) still represent notable case numbers but are lower in comparison, possibly due to either better access to safe water or smaller catchment populations. Clinics such as Mbare Polyclinic (45 cases), Mabvuku Polyclinic (23 cases), and Warren Park (13 cases) recorded fewer cases, which might suggest localized improvements in water quality or early health-seeking behavior, although underreporting cannot be ruled out.
The lowest number of cases (between 1 and 10) were reported at Hatcliffe Polyclinic, Avondale, Caledonia, Highfield Poly, Mabelreign, Gonda Hospital, Marlborough, and Glen Norah Sate, suggesting either effective disease control in these areas or underutilization of services and possible underdiagnosis. These patterns underline the importance of focusing public health interventions in high-burden suburbs, particularly in Mbare, Glen View, Budiriro, and Mufakose, where sanitation and water infrastructure are often strained. Surveillance should also be strengthened in areas with low reported numbers to rule out underreporting and improve outbreak detection and response.
Problem Statement
In recent years, the West South West and Southern districts of Harare in Zimbabwe experienced a significant surge in the number of reported typhoid fever cases. The problem was that every year there were reported increasing cases and recurring cases that catch health sector un prepared, ending up failing to prevent the disease to full capacity. This unexpectedly increased cases not only pose a serious risk to the health and well-being of the population but also places considerable strain on local healthcare resources and infrastructure. Despite previous efforts to manage and control typhoid outbreaks through public health interventions, the recent uptick indicated potential gaps in the existing prevention and response strategies. This study aimed to: 1: To predict typhoid fever outbreaks by predictive trends in Harare City typhoid hot areas. 2: To develop a mathematical model to simulate the spread of typhoid fever incidence under different intervention scenarios and recommend evidence-based strategies for reducing the disease burden in Harare City. By utilizing epidemiological data, this research seeks to provide a comprehensive Mathematical Model to analyze the future surge in typhoid cases, with the goal of informing actionable strategies and interventions that can effectively curb the outbreak and enhance public health resilience in the districts.
Figure 2. Trend of typhoid cases 2011 to January 2020
Download figure
Source: Author
Figure 2 shows fluctuations of cases. In 2018 and 2019 the graph is showing the highest cases to be recorded in a decade. From 2019 to 2020 there was a sharp decrease in cases , mainly due to 2019 targeted vaccination.
Literature Review
Typhoid fever remains a significant public health concern in many urban settings, particularly in low- and middle-income countries. Harare City, Zimbabwe, has experienced recurrent typhoid outbreaks, largely attributed to poor sanitation, contaminated water supplies, and socio-economic disparities. Mathematical modelling provides a robust framework for understanding the disease dynamics and evaluating the effectiveness of intervention strategies. In Harare City, Zimbabwe, an increase in cases from 2018 to 2020 highlighted the need for a deeper understanding of the driving factors behind these outbreaks (Pope, 2020).
Historical data indicate that Typhoid Fever is endemic in Zimbabwe, typically associated with periods of heavy rainfall and inadequate sanitation infrastructure (Chakuvinga P. e., 2017). The resurgence of cases in Harare during the specified period can be attributed to several factors, including urbanization, population density, and infrastructural challenges (Mavindu, 2018). A number of studies have identified key drivers responsible for the rise in Typhoid Fever cases. Poor water quality and sanitation are crucial factors in Typhoid transmission. Studies show that 80% of Typhoid cases are linked to contaminated water supplies (WHO, 2018). Harare's aging infrastructure has frequently resulted in sewer leaks and water contamination, as observed in outbreaks (Sokhela, 2019).
Environmental, Socio-Economic, and Demographic Drivers of Typhoid Fever Transmission: These factors determine the risk of exposure, the spread of infection, and the effectiveness of intervention measures. In Harare, rapid population growth, inadequate infrastructure, and climate variability exacerbate typhoid outbreaks. Understanding these drivers is critical for developing targeted interventions that reduce transmission and improve disease management.
Environmental Factors: Environmental conditions play a crucial role in the persistence and spread of Salmonella Typhi, the causative agent of typhoid fever. Poor water quality, inadequate sanitation, and seasonal variations contribute significantly to typhoid transmission. Studies have shown that contaminated water sources, including boreholes and open wells, are primary reservoirs of S. Typhi in endemic regions (Luby et al., 2019). Furthermore, seasonal rainfall has been linked to an increased incidence of waterborne diseases, as heavy rains facilitate the contamination of water supplies with fecal matter (WHO, 2018)
Socio-Economic Factors: Rapid urban population growth in Harare, combined with economic challenges, exacerbates the situation. Access to clean water and proper sanitation is often limited in high-density informal settlements (Davies, 2019). Research by Mhlanga et al. (2020) illustrates a direct correlation between socioeconomic status and incidence rates of Typhoid. Socio-economic disparities significantly influence the risk of typhoid infection. High-density suburbs in Harare, such as Mbare and Glen View, experience higher transmission rates due to overcrowding and inadequate waste disposal (MoHCC, 2020). Additionally, limited access to healthcare and delayed treatment-seeking behavior exacerbates disease burden, as undiagnosed cases continue to spread
the infection (Kariuki S, 2015). Informal food vending, common in urban markets, also plays a role in short-cycle transmission, as contaminated food and utensils facilitate the spread of S. Typhi (Dewan A, 2013).
Demographic Factors: Demographic characteristics such as age distribution, population mobility, and immunity levels influence typhoid transmission. Children and young adults are at a higher risk of infection due to increased exposure in schools and public spaces 11. Migration patterns in and out of Harare also impact disease persistence, as infected individuals may introduce new cases into different communities (Kim, 2019). Moreover, natural immunity following typhoid infection declines over time, necessitating booster vaccinations or repeated interventions (Andrews, 2019).
Behavioural Factors: Public WASH practices significantly influence the transmission dynamics of Typhoid Fever. A study by Ndlovu et al. (2019) found that inadequate handwashing and poor food handling practices are prevalent in affected communities, contributing to the persistence of the disease (Ndlovu, 2019).
Predicting Future Trends in Typhoid Fever Incidence: Mathematical modelling has been instrumental in predicting typhoid fever outbreaks and evaluating potential control strategies. Compartmental models such as the Susceptible-Infected-Recovered (SIR) framework have been widely used to simulate disease dynamics under different intervention scenarios (Pitzer et al, 2015). Recent studies have incorporated seasonal variations, antimicrobial resistance, and vaccination coverage to enhance model accuracy (Antillon et al, 2017). In the context of Harare, predictive models can be used to assess the impact of environmental and behavioural changes on future typhoid incidence.
One study conducted in sub-Saharan Africa demonstrated that improved water quality and sanitation could reduce typhoid incidence by up to 60% over a decade (Park et al., 2018). Similarly, vaccination campaigns targeting high-risk populations have been shown to provide significant long-term benefits, especially in endemic regions (Shakya et al, 2019). By integrating real-world data into mathematical models, policymakers can make informed decisions about resource allocation and disease control priorities.
Water, Sanitation, and Hygiene (WASH) Interventions: WASH interventions, including improved sanitation, water treatment, and hand WASH, have been widely recognized as effective measures for typhoid control. A systematic review by Balfour et al. (2021) found that access to clean water significantly reduced the risk of typhoid infection, with households using treated water experiencing a 40% lower infection rate compared to those relying on untreated sources. Furthermore, behavioural interventions such as community-led total sanitation (CLTS) programs have successfully reduced open defecation, thereby decreasing environmental contamination (Cairncross et al, 2010).
Vaccination Campaigns: Typhoid conjugate vaccines (TCVs) offer a long-lasting protective effect and have been recommended by the World Health Organization (WHO) for routine immunization in endemic areas. A randomized controlled trial in Nepal demonstrated that a single-dose TCV provided over 80% efficacy against typhoid fever over three years (Shakya et al, Efficacy of typhoid conjugate vaccine: A randomized controlled trial., 2021). Mathematical modeling studies have shown that incorporating TCVs into routine immunization schedules could lead to a substantial decline in typhoid incidence, particularly when combined with WASH interventions (Antillon et al, 2017). Between 2016 and 2019, Harare witnessed multiple typhoid outbreaks, with significant morbidity and mortality. These recurring outbreaks and the evolving problem of multidrug resistance (AMR) highlighted the urgent need for sustainable interventions to control the disease and prevent future epidemics. In response, the introduction of the Typhoid Conjugate Vaccine (TCV) was prioritized as part of a comprehensive strategy to combat typhoid fever by the Ministry of Health and Child Care (MOHCC) in February, 2019
Antibiotic Stewardship and Drug Resistance Management: The emergence of multidrug-resistant (MDR) S. Typhi strains poses a significant challenge to typhoid control efforts. In recent years, extensively drug-resistant (XDR) typhoid outbreaks have been reported in parts of Africa and South Asia, highlighting the need for improved antibiotic stewardship (Klemm et al, 2018). Surveillance data from Zimbabwe indicate a growing prevalence of resistant strains, necessitating the development of targeted treatment protocols and the promotion of rational antibiotic use (MoHCC, 2021). There is a need to understand the burden of typhoid fever in Harare and the effectiveness of TCV in mitigating outbreaks. Despite various interventions, typhoid remains a persistent health threat in the city, particularly in areas where there is inadequate sanitation.
Evaluating the trends and the effectiveness of TCV will provide critical insights to policymakers for refining vaccination strategies, enhancing public health interventions, and strengthening disease surveillance systems. This retrospective review aims to describe the epidemiology of typhoid outbreaks in selected suburbs of Harare from 2016 to 2024 and evaluate the effectiveness of the TCV campaign in reducing the typhoid disease burden in Harare City. By analyzing secondary data from health facilities and public health records, this study seeks to provide insights into the effectiveness of vaccination campaigns and inform future public health strategies. The findings will contribute to the growing body of evidence supporting the role of TCV in controlling typhoid fever in resource-limited settings
Conclusion: Mathematical modelling serves as a powerful tool for understanding typhoid transmission dynamics and evaluating intervention strategies. In Harare City, the integration of environmental, socio-economic, and demographic data into predictive models can enhance outbreak preparedness and response efforts. Evidence-based interventions such as WASH improvements, vaccination campaigns, and antibiotic stewardship programs offer promising pathways for reducing the disease burden. Future research should focus on real-time data integration and the development of adaptive models to address emerging challenges in typhoid control.
Materials and Methods
Study Design
The study employed secondary data analysis
Data Source and Study setting
We utilized data on microbiologically confirmed cases of Salmonella Typhi infection among patients seeking care at Beatrice Road Infectious Disease Hospital ( BRIDH) in Harare, Zimbabwe. This data was obtained from the City Health Departmental report of the cases line listed. The line list data was triangulated with data captured in the District Health Information System (DHIS2) for the same period. BRIDH is one of the two Infectious diseases hospitals in the City of Harare, providing free care for patients from Harare district and the surrounding towns. We had data on the aggregate number of S. Typhi isolates from January 2018 to January 2020 by patient age ( in 5 year age grouping). We also obtained demographic data on the population of Harare district (Harare Urban + Harare Rural) for the same period (Zimstats, 2022)
Attack Rate
This refer to the proportion of individuals who become ill during an outbreak or specific time period, and it is calculated as:
Attack Rate = Number of new cases of disease in a population/Total population at risk during the specific time period* 100,000
This rate allows for easy comparisons between populations. Attack rates aids in identifying the severity of an outbreak and can be used to assess the effectiveness of interventions, such as vaccination campaigns
Study Settings and Study Population
The study was conducted in Harare City. Harare City has a population of 1 846 437 (ZIMSTATS, 2022). During the time of the outbreak Harare City was made up of eight (8) districts. The outbreak was mainly confined to the West South West and Southern districts. In that regard this study will only focus on these two hotspot districts. The areas sampled for the study purposes are Mbare, Waterfall, Glen View, Mufakose and Budiriro suburbs. The total population for the sampled suburbs is 453 245 and a total of 2341 confirmed cases reported. The study was carried out using data collected electronically from linelists from the City’s Health Information Unit.
Model development
We developed and modified a dynamic compartmental SIR-based model to simulate typhoid transmission through both direct human-to-human contact and environmental pathways. The methodology involved the following approaches:
· Model Calibration: The model was calibrated using surveillance data from Harare (2018–2020) by adjusting transmission parameters to fit observed case trends.
· Model Validation: Validation was performed by comparing model outputs against independent data, ensuring the model accurately captured the disease dynamics.
· Model Fitting: The model was fitted using statistical techniques to minimize discrepancies between simulated and reported case counts, verifying accuracy through goodness-of-fit metrics.
· Scenario Analysis: Different intervention scenarios, including targeted vaccination in high-risk areas, were simulated to assess their impact on transmission reduction.
· Sensitivity Analysis: Key model parameters were varied systematically to determine their influence on disease dynamics and to assess model robustness.
· Case Prediction: The model projected future case trends under different intervention strategies, allowing for comparative assessment of potential outbreak control measures.
Model Description
We adapted a previously developed mathematical model for the transmission dynamics of typhoid in Malawi 8 by fitting to the data from BRIDH and modifying the model to explore hypotheses for the increase in typhoid fever cases beginning in 2018. The model is illustrated in Figure 1 below. The model assumes that individuals are born susceptible to infection and disease caused by Salmonella Typhi (S1). The susceptible persons are infected at a rate (λp + λw) that is mediated through contaminated food and water in the immediate environment (“short-cycle transmission,” λp) as well as bacterial contamination of water supplies and the broader environment (“long-cycle transmission,” λw). Individuals experiencing primary infection (I1) remain infectious for a period 1/δ, after which we assume a fraction (α) experience disease-induced mortality, a fraction (θ) develop an infection of the gallbladder and become chronic carriers (C), and the remaining individuals (1-θ-α) recover and are temporarily immune (R). We assume that θ depends on the age of the infected person, consistent with epidemiological data 8. Immunity to reinfection wanes at a rate ω, leaving the individual partially susceptible (S2). If reinfection occurs prior to waning of partial immunity (at a rate ϵ), we assume these reinfections (I2) are subclinical and are not reflected in our data. Sub-clinically infected individuals can again recover or become chronic carriers. Additional dynamics include susceptible individuals that get vaccinated (V) at a rate τ. The infectious individuals shed bacteria into the environmental reservoir (W). We assume all infectious individuals shed bacteria into the environmental reservoir (W) at a rate γ, and the bacteria remain infectious for a period 1/ξ. Both chronic carriers and subclinically infected individuals have infectiousness reduced by a factor r. For the compartmental mathematical model for the transmission dynamics of typhoid, we assumed that short-cycle transmission was contact frequency dependent and mixing was homogeneous while long-cycle transmission depended on both contact frequency and population density. Frequency-dependent transmission was applied in settings where water sources are shared by a fixed number of individuals, such as households or small communities. In modeling the transmission dynamics of typhoid, we assume that short-cycle transmission (e.g., within households or small communities) follows a frequency-dependent pattern with homogeneous mixing. This means that infection risk is based on how often individuals come into contact with contaminated food, water, or fomites, rather than the total population size. Since these interactions occur in smaller, well-connected groups, every susceptible individual has a similar probability of exposure. This assumption aligns with real-world scenarios where water sources are shared by a fixed number of individuals, making contact frequency the key determinant of transmission.
In contrast, long-cycle transmission (e.g., through urban water supplies, rivers, or reservoirs) is modeled as density-dependent, meaning infection risk increases with population size. This reflects the reality that larger populations contribute more bacteria to shared water sources and have a greater likelihood of exposure. The choice between frequency-dependent and density-dependent transmission depends on the scale of bacterial contamination and epidemiological context. By incorporating both transmission pathways, the model provides a more accurate representation of typhoid spread, helping to design effective public health interventions such as household water treatment and large-scale sanitation improvements.
In contrast, density-dependent transmission was used to model scenarios where larger populations contribute to and are exposed to a common water reservoir, such as urban water supplies or rivers. The choice of transmission mode depended on the specific epidemiological context and scale of bacterial contamination. Finally, there are three model assumptions which are homogeneous mixing within each population, Constant recruitment rate (B) into the susceptible compartments, Natural mortality occurs at rate μ in all compartments (Figure 3).
Figure 3. Compartmental diagram of model structure. Source: (Adapted from Pitzer VE, 2014)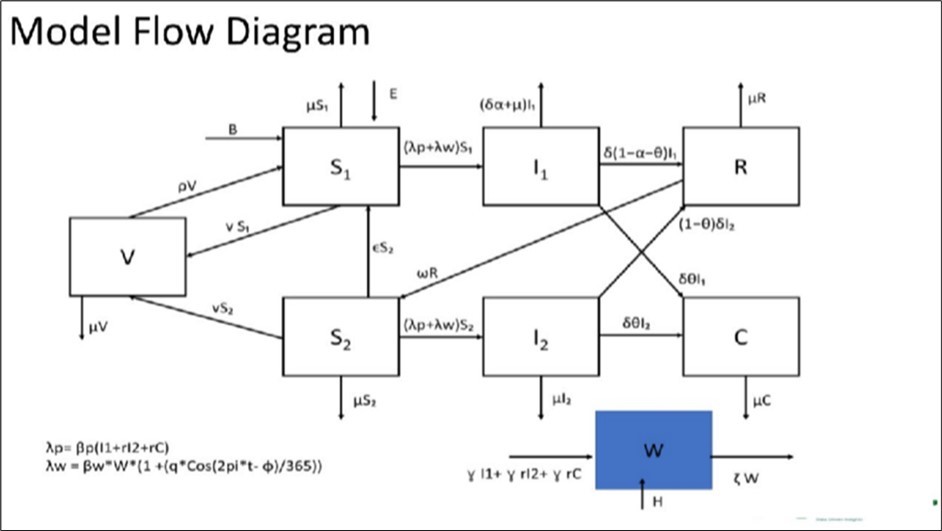
Download figure
Variables, and Parameters.
| C | Chronic disease (career) population. |
| W | environmental reservoir |
| X | susceptible individuals that develop cross-protective immunity |
| V | Represents the flow of individuals from the vaccinated (immune) compartment back to the susceptible class due to waning immunity. It models waning vaccine-induced immunity over time, whereby vaccinated individuals gradually become susceptible again. |
| Observed cases | Reported cases derived from infected compartments. |
Model Parameters, Descriptions, Estimates, Sources, and Estimation Methods
| Parameter | Parameter | Estimate | Source | Estimation Method Used |
| B | Birth rate | 27/1000 | ZIMSTATS (Zimbabwe National Demographic Data) | Direct demographic data (empirical) |
| μ | Natural mortality rate | 7.4/1000 | ZIMSTATS (Zimbabwe National Demographic Data) | Direct demographic data (empirical) |
| 1/δ | Rate of leaving the Infectious compartment | 1/7 days = 0.1429 | Estimated from clinical typhoid data | Empirical estimation from clinical recovery duration |
| α | Fraction of infected individuals who die from the disease | 0.0029 | Estimated from clinical typhoid data | Empirical estimation from clinical cas fatality data |
| θ | Fraction of infected individuals who become chronic carriers | 0.02 | Estimated from clinical typhoid data and literature | Literature- informed empirical estimate |
| 1/ω | Rate of waning immunity | 0.33 | Estimated based on immune waning studies and literature | Bayesian estimation calibrated withliterature priors |
| ϵ | Rate of becoming fully susceptible again | 0.1 | Estimated from literature and localdata (WHO, 2023) | Literature- informed empiricalestimate |
| γ | Rate of bacterial shedding into the environment | 1 infectiousunit per week | Estimated frommicrobiological studies of carriers | Literature-based empirical estimate |
| r | Reduction factor in infectiousness for chronic carriers and subclinical infections | 0.3 | Estimated from studies on chronic carriers’ infectivity | Literature-based empirical estimate |
| ξ | Rate of bacterial decay in theenvironment | 1/3 per week | Pitzer et al. (2014) | Literature-based fixed estimate |
| βp | Short-cycle transmission coefficient | 0.0001 | Estimated via model fitting to case data | Maximum Likelihood Estimation (model calibration) |
| βw | Long-cycle transmission coefficient | 0.0005 | Estimated via model fitting; calibrated to observed trends | Maximum Likelihood Estimation (model calibration) |
| q | Seasonal variation amplitude | 0.5 | Estimated from seasonal case data | Model fitting using Maximum Likelihood Estimation |
| φ | Phase shift for seasonal transmission | 0 | Estimated during model fitting | Model fitting (MLE) |
| e | Education coverage | 0.3 | Estimated and assumed from intervention coverage data | Empirical assumption based on program data |
| h | WASH interventions | 0.5 | Estimated from programimplementation data | Empirical estimate from intervention reports |
| ρ | Rate of loss of vaccine immunity rate | 0.33 | Estimated based on vaccine efficacy studies | Bayesian estimation based on vaccine immunity decay literature |
Parameter Derivation Summary
Parameter values were derived from a combination of empirical data, published literature, and model calibration procedures to ensure biological and epidemiological realism. Demographic parameters such as the birth rate (B) and natural mortality rate (μ) were obtained directly from ZIMSTATS national demographic data (2023). Clinical parameters including the infectious period (1/δ), disease fatality rate (α), and fraction progressing to chronic carriage (θ) were empirically estimated from hospital and surveillance data and cross-validated with published clinical studies of typhoid in sub-Saharan Africa (Table 1).
Parameters associated with immunity dynamics, such as the rate of waning immunity (ω), return to full susceptibility (ε), and loss of vaccine-induced immunity (p), were derived from immunological and vaccine efficacy studies, supported by WHO (2023) reports and regional serological data. These were fine-tuned through Bayesian posterior estimation and Maximum Likelihood Estimation (MLE) techniques to improve model fit to observed typhoid trends.
Environmental and transmission-related parameters including short-cycle (βp) and long-cycle (βw) transmission coefficients, bacterial decay rate (ξ), and reduction factor in infectiousness (r) were estimated via model fitting and calibration using reported typhoid case time series. Literature sources such as Pitzer et al. (2014) informed plausible ranges. Intervention coverage parameters (education e, WASH h) were estimated from program implementation data and public health reports in Zimbabwe.
This mixed approach integrating empirical data, literature-informed priors, and formal parameter estimation ensured that model parameters reflected both local epidemiological conditions and globally recognized biological constraints, thereby improving the robustness and interpretability of the simulation outcomes (Table 3).
Table 3. Intervention parameters| Intervention parameters | Description | Estimate |
| edu_start_time | Health education starts after 1 year | 365 * 1 |
| edu_coverage | 70% coverage | 0.7 |
| edu_efficacy | 50% reduction in transmission | 1 |
| wash_start_time | WASH intervention starts after 2 years | 365 * 2 |
| wash_coverage | 80% coverage | 0.8 |
| wash_efficacy | 60% reduction in environmental transmission/shedding | 0.6 |
| v | Vaccination rate | 0.05 |
Differential Equations:
Susceptible individuals (S₁)
dS₁/dt=B−(λp+λw)S₁−μS₁+ϵS₂ - v S₁ +ρV
B: Birth rate of susceptible individuals.
λp: Rate of short-cycle transmission.
λw: Rate of long-cycle transmission.
μ: Natural mortality rate.
ϵ: Rate at which partially immune individuals become fully susceptible again.
v : Vaccine rate
ρ: Rate at which individual lose vaccination immunity
Primary infected individuals (I₁)
dI₁/dt=(λp+λw)S₁−(δα+μ)I₁−δ(1−α)I₁−δθI₁
δ: Rate at which infected individuals leave the infectious compartment.
α: Fraction of infected individuals who experience disease-induced mortality.
θ: Fraction of infected individuals who become chronic carriers.
Recovered individuals (R)
dR/dt=δ(1−α−θ)I₁ +(1−θ)δII₂−ωR−μR
ω: Rate at which immunity wanes.
Partially susceptible individuals (S₂)
dS₂dt=ωR−(λp+λw)S₂−μS₂−ϵS₂-vS₂
Subclinically infected individuals (I₂)
dI₂/dt=(λp+λw)S₂ − (1−θ)δII₂ - δθI₂ - μI₂
Chronic carriers (C)
dC/dt = δθI₁ + δθI₂−μC
Environmental reservoir of bacteria (W)
dWdt = γ(I₁ +rII₂+rC)−ξW
r: Reduction factor in infectiousness for chronic carriers and subclinically infected individuals.
ξ: Rate at which bacteria in the environment lose infectivity.
γ: Rate at which infectious individuals shed bacteria into the environment.
Vaccination (V)
dV/dt = v S₁ + vS₂ - ρV- μV
Transmission Rates
· Short-cycle transmission (λp)
λp=βp(I1+rI2+rC)
βp: Transmission coefficient for short-cycle transmission.
· Long-cycle transmission (λw)
λw=βwW(1+qcos((2πt−φ)/365))
βw: Transmission coefficient for long-cycle transmission.
q: Amplitude of seasonal variation.
Model Scenarios for Typhoid Emergence at BRIDH
Scenario 1: Treatment Only
This scenario explores the impact of clinical treatment alone on reducing typhoid burden. All infected individuals who seek care are assumed to receive effective antibiotic treatment. We model reduced infectious duration and decreased transmission, assuming treatment success is uniform across the population.
Scenario 2: Treatment + Vaccination
This scenario incorporates both treatment of clinical cases and typhoid conjugate vaccine (TCV) rollout. Vaccination reduces susceptibility among the immunized and indirectly lowers transmission. We assume a given vaccine efficacy and coverage rate, with parameter estimation including vaccine-induced immunity duration.
Scenario 3: Treatment + WASH (Water, Sanitation, and Hygiene)
We evaluate the joint impact of clinical treatment and improved WASH infrastructure. WASH interventions reduce long-cycle transmission by lowering environmental contamination. This scenario assumes partial coverage of WASH improvements across the population and estimates corresponding reductions in transmission parameters.
Scenario 4: Treatment + Typhoid-related Health Education
This scenario assesses the effect of treatment combined with public health education focused on typhoid prevention behaviors (e.g., handwashing, safe food practices). The education component is modeled as reducing the effective contact rate for short-cycle transmission.
Scenario 5: Treatment + WASH Only
Here, we re-express the Treatment + WASH scenario assuming only partial or localized WASH coverage, to reflect implementation in limited settings such as schools or high-risk neighborhoods. We assess whether small-scale WASH improvements, together with treatment, still meaningfully impact transmission.
Scenario 6: Treatment + WASH + Vaccination
This scenario explores a comprehensive intervention involving treatment, vaccination, and WASH improvements. We estimate the synergistic effects of reducing susceptibility, infectiousness, and environmental contamination.
Scenario 7: Treatment + WASH + Typhoid-related Health Education
In this scenario, we assess the combination of treatment, WASH, and behavior change communication campaigns. The model incorporates changes in both environmental and behavioral drivers of transmission, estimating their joint impact on typhoid dynamics.
Scenario 8: Full Integrated Intervention (Treatment + WASH + Vaccination + Typhoid- related Health Education)
This scenario models the full suite of interventions implemented concurrently. It provides an upper-bound estimate of potential typhoid control, integrating medical, infrastructural, and behavioral approaches. We evaluate the combined effects on both short-cycle and long-cycle transmission pathways.
Model Fitting
We fitted our model to the data on culture-confirmed cases of S. Typhi at BRIDH from 2018 to 2020 by maximum a posteriori estimation. We assumed uniform prior distributions for all model parameters (Table 2). We calculated the log-likelihood of each model assuming that the weekly number of observed cases in each age group is Poisson-distributed with a mean equal to the
model-predicted number of clinical infections over the duration of infectiousness times the reporting fraction, f. Because we only have data on the age of cases beginning in 2018, we fit the model to the data up to 2018 by summing the model-predicted number of cases each week across all age groups. We will calculate the Bayesian information criterion (BIC) for each best-fit model to compare models with a different number of estimated parameters across the different scenarios (Table 2).
Sensitivity Analysis
Figure 4. Sensitivity Analysis (Interventions)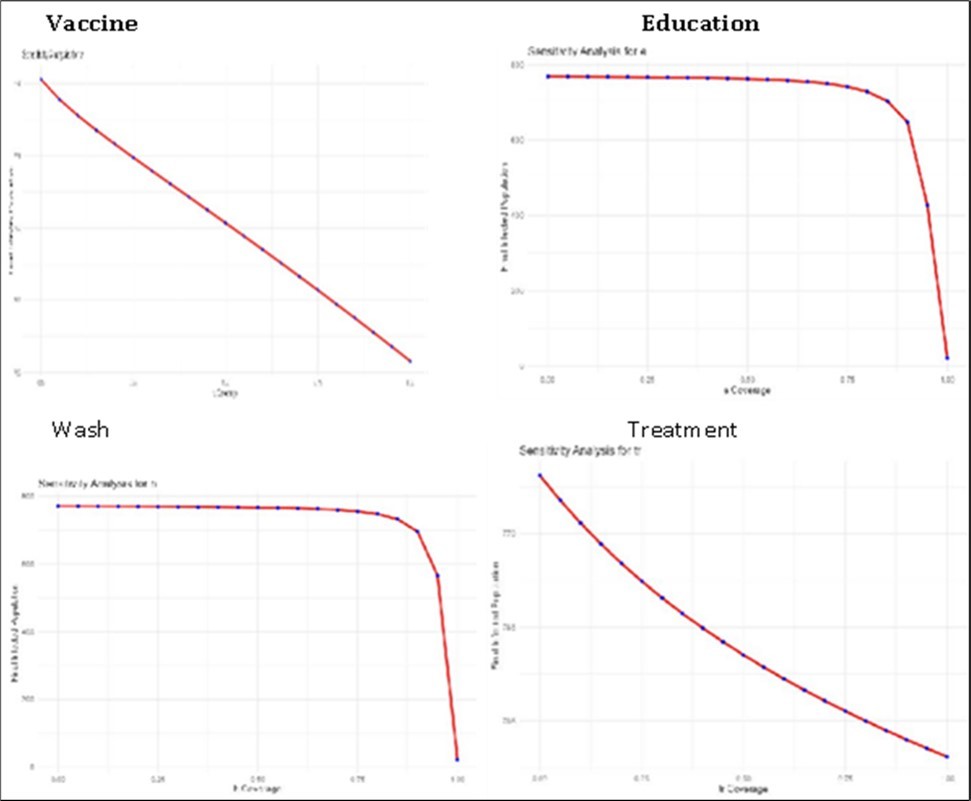
Download figure
From the Graphs (Figure 4) above it seems as Vaccine, Education and wash start to make significant changes or start to be more sensitive at 87% however treatment shows to be very sensitive from small changes.
Results
This chapter presents the results obtained from the epidemiological model assessing the impact of susceptibility, infection, recovery, chronic carriers, and intervention strategies on the dynamics of typhoid transmission. The results are structured based on model simulations, intervention comparisons, and key epidemiological outcomes. Of the microbiologically confirmed cases (2341) there was no significant difference in numbers between Males and Females. Those aged 16 and below exemplified the highest attack rate as compared to those above 16 years of age. Of the 2341 confirmed cases the majority came from Glen View and Budiriro suburbs i.e. 36% and 29% respectively. A two-week TCV campaign introduced in February 2019 had high vaccine coverage with an average of 85%.
Overview of the Trends and Predictive Model
Figure 5. Average Fitted Histogram (Observed and fitted)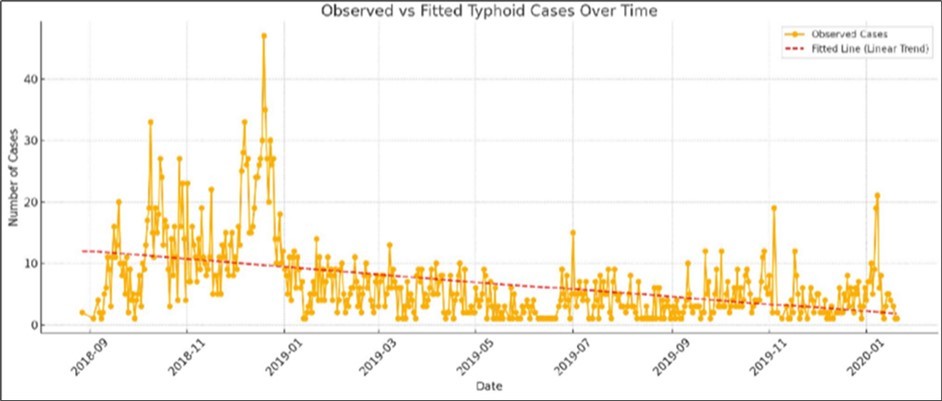
Download figure
According to the graph (Figure 5) after average fitting Most cases recorded are from September 2018 to January 2019.Then from that cases were decreasing. The red dotted line shows that on average cases were decreasing from January 2019. The epidemic curve shows cases by date of onset from 2018 to January 2020. The highest peak of cases was recorded in December 2018. Mass vaccination started on February 15, 2019 for two weeks. Just over half of the cases (56%) were reported before TCV.
Figure 6. Fitted Model & Average Forecasting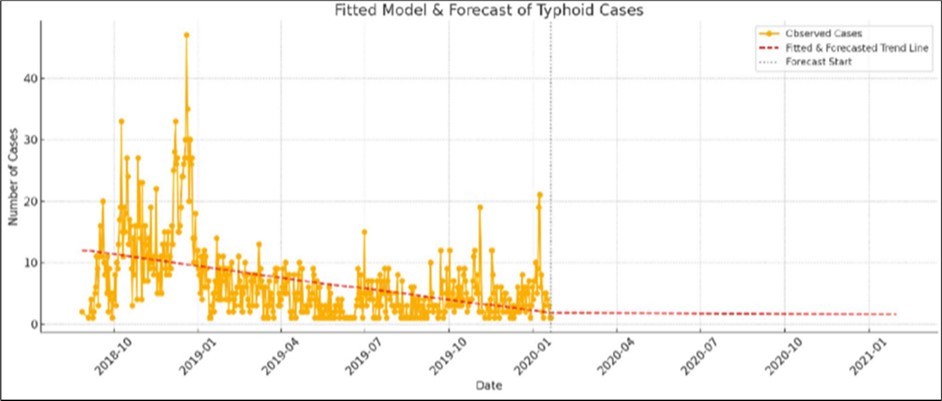
Download figure
Using the data from 2018 to 2020, the forecast predicted a decrease and constantly low number of cases, however as of 2025 we have experienced increasing cases. This could have been attributed to the waning immunity of the Typhoid Conjugate Vaccine (TCV) administered in 2019 in these hotspots.
Scenario Analysis
Figure 7. Health education and Wash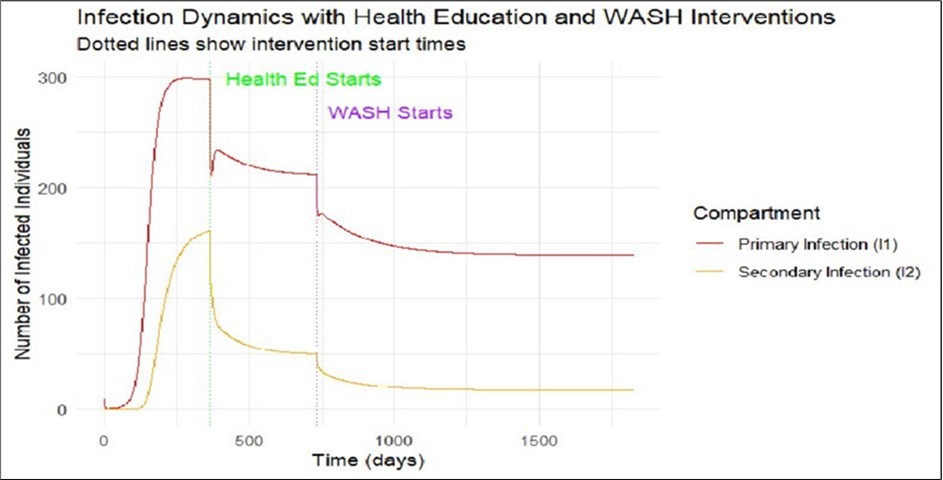
Download figure
In the primary infection model, the scenario with treatment alone results in a dramatic increase in cases, reaching approximately 300 within less than a year. However, when typhoid-related health education is introduced, the number of infections drops significantly to around 223. The addition of WASH interventions further reduces the burden, bringing primary infections down to approximately 140 cases. A similar trend is observed with secondary infections: without any intervention, secondary cases reach around 165. Following the introduction of health education, this number decreases sharply to 50, and further declines to 20 after the implementation of WASH interventions. These results highlight the substantial impact of layered public health interventions in reducing both primary and secondary typhoid infections (Figure 7).
Figure 8. Vaccination, Health education and Wash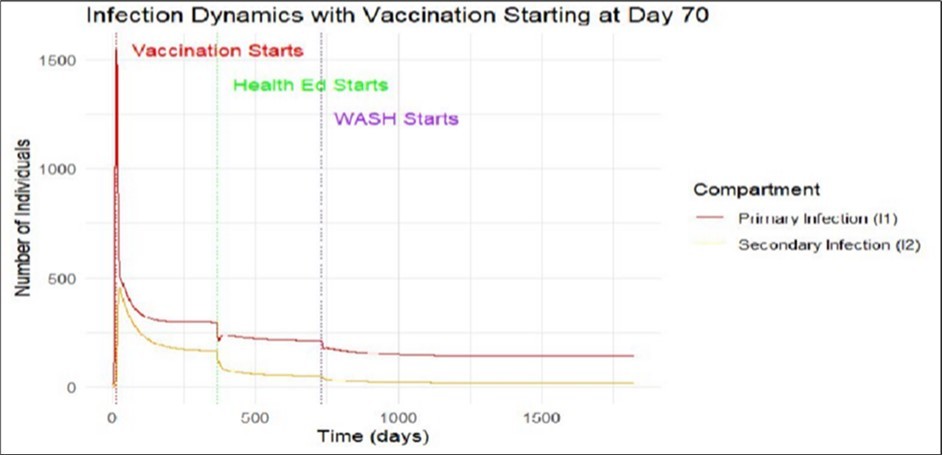
Download figure
In the primary infection model, the introduction of vaccination leads to a sharp and rapid decrease in infections, dropping from approximately 1,500 to around 500 cases within a few days. Following this, the implementation of typhoid-related health education results in a more gradual decline, with cases falling to about 245 within less than a year. The subsequent introduction of WASH interventions further reduces the number of primary infections to approximately 125. A similar pattern is observed for secondary infections: under vaccination alone, cases drop from 485 to 125. With the addition of health education, secondary infections fall to fewer than 25, and after the implementation of WASH interventions, the number declines even further to fewer than 10. These findings underscore the cumulative benefits of combining vaccination with health education and WASH in effectively controlling typhoid transmission (Figure 8).
Figure 9. Environmental Pathogen and Chronic infection with Wash Interventions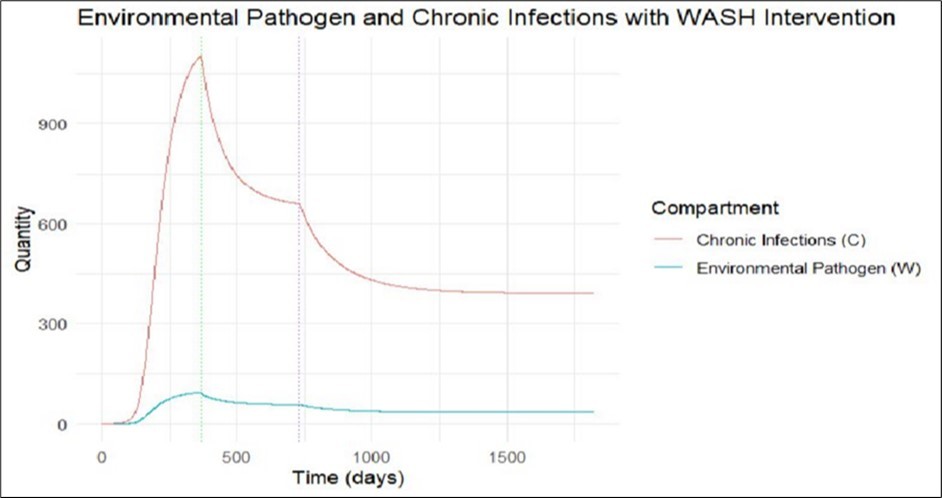
Download figure
The graph (Figure 9) demonstrates a significant decline in both environmental pathogens and chronic infections following the implementation of each intervention. The number of chronic carriers drops markedly, primarily due to the impact of improved WASH interventions, which effectively reduce long-cycle environmental transmission (λw). This emphasizes the vital role of environmental sanitation in breaking the transmission cycle and reducing the reservoir of chronic carriers in the population. In the absence of interventions, chronic infections reach approximately 1,100 cases. With the introduction of health education, this number decreases to around 650, and further declines to about 400 after implementing WASH. Similarly, environmental pathogen levels show a dramatic reduction—nearly 75%—once both health education and WASH interventions are introduced (Figure 10).
Figure 10. Optimum Scenario: Projected intervention coverages > 70% for all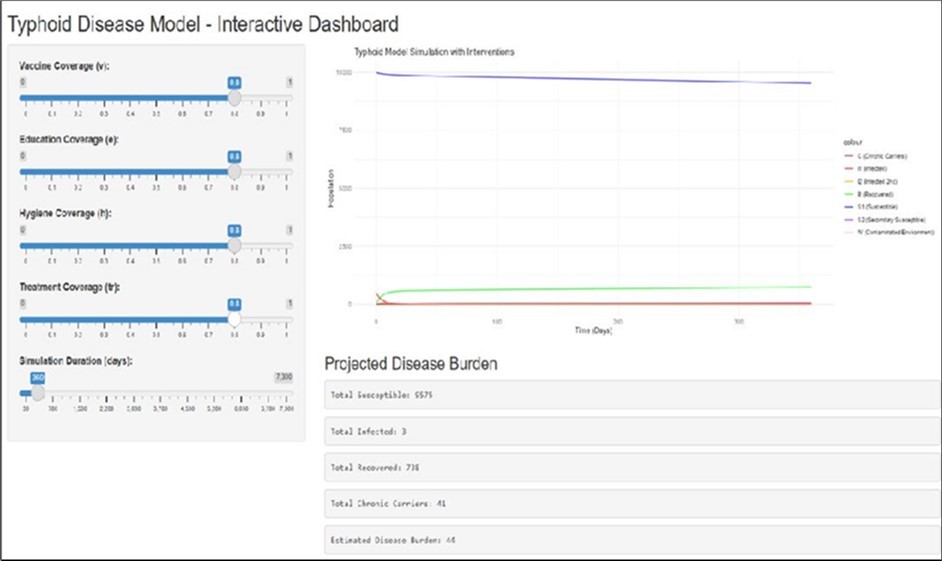
Download figure
The dashboards are capable of displaying all scenarios, with adjustments made according to the selected interventions. This particular graph demonstrates the simulation of various interventions to determine their optimal impact. Additionally, the same dashboards can predict the total number of infections over time under different intervention strategies. In this case, the model predicts only three infections 360 days after the start of 2020, which closely aligns with the average trend depicted in Figure 6.
Summary of Findings
This study set out to predict future trends in typhoid fever cases in the hotspot areas of Harare City and to develop a mathematical model that simulates the spread of typhoid under varying intervention scenarios. The analysis of data from 2018 to 2020 revealed that the majority of typhoid cases occurred between September 2018 and January 2019. Following this peak, the fitted trend line showed a consistent decline in cases, particularly after January 2019. Forecasts based on this
historical data predicted a continued decrease and a persistently low number of cases into the future. However, real-world observations in 2025 show a concerning resurgence of cases, suggesting that immunity from the Typhoid Conjugate Vaccine (TCV), widely administered in 2019, may have waned over time, leaving the population vulnerable once again.
The simulation of intervention scenarios using the mathematical model further highlighted the differential impact of various strategies on primary and secondary infections. When treatment alone was applied in the primary infection model, there was a sharp increase in cases, reaching approximately 300 within less than a year. The inclusion of typhoid-related health education, however, resulted in a substantial reduction in cases to around 223. The addition of WASH interventions had a further suppressive effect, lowering infections to about 140. A similar trend was observed for secondary infections: from an estimated 165 cases without intervention, health education reduced this figure to 50, and WASH interventions brought it down even further to 20.
Moreover, the model that incorporated vaccination demonstrated a rapid and significant drop in infections. Primary infections fell from approximately 1,500 to 500 within days following vaccination. Health education and WASH interventions layered on top of vaccination continued to drive infections downward, reaching around 245 and 125 respectively. The same was seen with secondary infections, which decreased from 485 to 125 with vaccination alone, then declined to under 25 with health education, and ultimately fell to fewer than 10 with full intervention layering.
The simulations also assessed the impact of interventions on environmental pathogens and chronic infections. Without any interventions, chronic infections rose to around 1,100 cases. Health education led to a drop to 650, while WASH interventions further reduced this to 400. Environmental pathogen levels followed a similar trajectory, with a near 75% reduction when both health education and WASH strategies were implemented. Dashboards developed in this study allowed real-time scenario simulation and visualization of intervention impacts, predicting as few as three cases 360 days after the start of 2020 in a full-intervention scenario—closely aligning with trends depicted in the models.
Discussion
The results of this study provide meaningful insights into the dynamics of typhoid fever transmission in Harare City and demonstrate the relative effectiveness of various public health interventions. The observed decline in cases between 2019 and 2020 aligns with the introduction of the Typhoid Conjugate Vaccine (TCV), which had been rolled out in Harare’s hotspot areas. This finding is consistent with studies by Qadri et al. (2021), who reported significant short-term reductions in typhoid incidence following mass TCV campaigns in South Asia. Similarly, Voysey et al. (2020) noted a marked decline in typhoid incidence within the first year post- vaccination in Malawi, another sub-Saharan African context, highlighting the vaccine's efficacy during initial implementation.
However, unlike these earlier studies which focused primarily on the immediate post-vaccination impact, this study projects beyond the short term and provides evidence of a resurgence in cases by 2025. This finding suggests that vaccine-induced immunity may wane over time, especially in the absence of booster doses or sustained public health infrastructure. These results are aligned with findings by Shakya et al. (2022), who cautioned that immunity from a single dose of TCV may decline after three to five years, especially in endemic settings. Therefore, the observed rise in cases in Harare’s hotspot areas reinforces the importance of ongoing surveillance and long- term vaccination strategies.
The modeling of different intervention scenarios highlighted the critical need for a multi-pronged approach. The limited effect of treatment alone reflects observations from Kim et al. (2019), who argued that relying solely on antibiotic therapy in endemic regions does little to prevent transmission due to the presence of asymptomatic carriers and environmental reservoirs. In contrast, this study found that integrating health education and WASH (Water, Sanitation, and Hygiene) interventions significantly reduced both primary and secondary infections. This aligns with the findings of Azman et al. (2018), who emphasized the impact of WASH interventions in reducing enteric infections and called for their prioritization alongside vaccination in urban slums and informal settlements.
The simulation results also revealed that vaccination, when layered with health education and WASH interventions, yields the most dramatic and sustained reduction in typhoid cases. This cumulative impact supports the framework proposed by Antillon et al. (2017), who modeled
cost-effective combinations of typhoid control strategies and concluded that integrated approaches offered the greatest long-term benefits in low-resource settings. Furthermore, the steep reductions in environmental pathogen levels and chronic carrier prevalence following WASH implementation are consistent with the environmental modeling work of Pitzer et al. (2014), who demonstrated that reducing environmental contamination significantly lowers long- cycle transmission.
Incorporating interactive dashboards into the study added practical value, allowing for visualization of intervention outcomes and real-time forecasting. This approach echoes the recommendations by Stanaway et al. (2019), who advocated for the integration of dynamic modeling tools into public health decision-making frameworks to better tailor responses in rapidly changing epidemiological contexts.
Overall, while the findings corroborate much of the existing literature on the benefits of vaccination, WASH, and health education, this study contributes a unique longitudinal modeling perspective that not only confirms the short-term effectiveness of interventions but also demonstrates the potential for disease resurgence if efforts are not sustained. This reinforces the call by Mogasale et al. (2020) for continuous monitoring and adaptation of typhoid control programs, particularly in urban African settings.
Study Limitations
The model described in the manuscript offers a structured approach to understanding typhoid transmission dynamics and intervention impacts. However, like all models, it has certain limitations that could affect its accuracy and applicability. Some key limitations have been identified:
In terms of Homogeneous Mixing the model likely assumes that individuals mix uniformly within the population, which may not reflect real-world social, geographic, or behavioral heterogeneity. Many parameters are assumed constant over time, ignoring seasonal or temporal variations in transmission, behavior, or intervention coverage. The model does not explicitly account for age-specific differences in susceptibility, exposure, or immunity, which are important in typhoid epidemiology. Some parameters were estimated from literature and limited local data, which could introduce inaccuracies. Typhoid case data usually suffer from
underreporting, misclassification, and diagnostic limitations, affecting model calibration and validation.
The model assumed static coverage levels for interventions like vaccination, WASH, or education, whereas in reality these change over time. The model also simplified immunity waning and vaccine efficacy, which can vary among individuals and over time. While carriers were included, the complexity of chronic carriage, including variable infectivity and potential for reactivation, may be oversimplified. The environmental transmission was modeled with a decay rate, but spatial heterogeneity and environmental complexities are not explicitly represented. The model did not incorporate spatial heterogeneity or social networks, which can significantly influence transmission dynamics, especially in urban vs. rural settings. Finally the model may not account for population movement, importation of cases, or cross-border transmission, which can affect local dynamics or potential changes in pathogen characteristics that could influence transmission or treatment outcomes.
While the model provides valuable insights into typhoid dynamics and potential intervention impacts, its limitations stem mainly from simplifying assumptions, data uncertainties, and lack of detailed heterogeneity. Recognizing these limitations is crucial for interpreting the results and guiding real-world decision-making. Future enhancements could include incorporating spatial structure, age stratification, behavioral factors, and stochasticity to address some of these constraints.
Conclusion
This study provides a comprehensive analysis of typhoid fever trends in Harare City’s hotspot areas, offering valuable insights into the effectiveness of different public health interventions in controlling the disease. The findings confirm that while the Typhoid Conjugate Vaccine (TCV) administered in February 2019 initially led to a reduction in cases, immunity may wane over time, leading to a resurgence in infections as observed in 2025. This emphasizes the need for booster vaccinations or alternative interventions to sustain control efforts.
The mathematical model used in this study demonstrated that interventions such as health education and WASH (Water, Sanitation, and Hygiene) significantly reduce both primary and secondary infections, with a layered approach yielding the most effective results. Vaccination, in
combination with these preventive measures, was found to be the most powerful strategy in reducing disease burden, supporting the growing body of literature advocating for integrated public health approaches.
Furthermore, the study underscored the importance of addressing environmental transmission and chronic infections, which are often overlooked in traditional typhoid control strategies. The role of environmental sanitation, particularly through WASH interventions, was pivotal in reducing long-term transmission cycles and chronic carrier prevalence, highlighting the necessity of improving sanitation infrastructure in endemic regions.
Overall, the study reaffirms the importance of a multifaceted, sustained, and adaptable approach to typhoid control, one that incorporates vaccination, health education, and environmental improvements. It also emphasizes the need for ongoing surveillance to monitor the effects of vaccination and interventions over time, as well as the necessity of adapting strategies to account for potential shifts in the epidemiological landscape, as observed in Harare.
Recommendations
· Booster Vaccination Programs: Given the observed decline in immunity over time and the resurgence of cases in 2025, it is recommended that booster vaccination campaigns be implemented in hotspot areas. Continuous monitoring of vaccine efficacy should inform the need for additional doses, particularly in regions with high transmission rates. Future vaccination efforts should be integrated into routine immunization schedules to maintain high levels of community immunity over the long term.
· Integrated Public Health Interventions: The study highlights the effectiveness of combining vaccination, health education, and WASH interventions to reduce the burden of typhoid fever. It is recommended that health education campaigns focus on promoting hygiene practices, safe water use, and proper sanitation, particularly in urban slums and informal settlements. These educational efforts should be coupled with the widespread availability of safe water and improved sanitation infrastructure to address environmental transmission risks.
· Strengthening WASH Infrastructure: The reduction in chronic infections and environmental pathogen levels following WASH interventions underscores the need to invest in improved water, santation, and hygiene infrastructure. Local governments should prioritize water treatment, sewage systems, and waste disposal improvements, particularly in high-risk communities, to break the transmission cycle of typhoid fever. Additionally, community-based sanitation programs should be supported to ensure sustainability and community ownership of WASH facilities.
· Enhanced Surveillance Systems: Continuous surveillance of typhoid fever cases is essential to monitor trends and identify potential outbreaks in real-time. Surveillance systems should integrate data from hospitals, clinics, and environmental health programs to allow for a comprehensive understanding of the disease’s dynamics. This data can inform public health responses and allow for timely adjustments to intervention strategies.
· Research on Long-Term Vaccine Efficacy: Further research is needed to assess the long-term effectiveness of the Typhoid Conjugate Vaccine (TCV) in different populations. Longitudinal studies should focus on tracking immunity over time and identifying potential gaps in protection. Research should also explore alternative vaccines or formulations that may offer longer-lasting immunity.
· Community Engagement and Participation: Community involvement in health education and disease prevention efforts is critical for the success of typhoid control programs. Local leaders and community groups should be engaged to help disseminate information and encourage participation in vaccination and hygiene initiatives. This can help overcome barriers to intervention acceptance and ensure that public health campaigns are culturally appropriate and widely adopted.
· Intervention Modeling for Policy Decision-Making: Policymakers should utilize mathematical modeling tools, such as those employed in this study, to evaluate the potential impact of different intervention strategies and predict future disease trends. These tools can assist in optimizing resource allocation, ensuring that public health interventions are both cost-effective and tailored to the specific needs of affected communities.
References
- 2.Mogasale V, B M. (2014) Burden of typhoid fever in low-income and middle-income countries: a systematic, literature-based update with risk-factor adjustment. Lancet Glob Heal. 570-80.
- 4.Feasey N A, K G. (2015) Rapid emergence of multidrug resistant. H58-lineage Salmonella typhi in Blantyre, Malawi. . PLoS Negl Trop Dis, 9:e0003748 .
- 5.Holt K E, M P. (2011) Emergence of a globally dominant IncHI1 plasmid type associated with multiple drug resistant typhoid. , PLoS Negl Trop Dis 5.
- 7.Wong V K, S B. (2015) WonPhylogeographical analysis of the dominant multidrug- resistant H58 clade of Salmonella Typhi identifies inter- and intracontinental transmission events. , Nat Genet 47, 632-9.
- 8.Pitzer V E, C B. (2014) Predicting the impact of vaccination on the transmission dynamics of typhoid in South Asia: a mathematical modeling study. PLoS Negl Trop Dis.
- 9.Ames W R, M R. (1943) Age and sex as factors in the development of the typhoid carrier state, and a method for estimating carrier prevalence. , Am J Public Health 33, 221-30.
- 10.Baker S, P D. (2013) Fitness benefits in fluoroquinolone-resistant Salmonella Typhi in the absence of antimicrobial pressure. , eLife 1-17.
- 11.J A Crump, E D Mintz. (2020) Global trends in typhoid and paratyphoid fever. The Lancet Infectious Diseases. 20(3), 242-243.
- 13.N C Lo. (2021) Typhoid vaccine introduction: Impact and cost-effectiveness. , The Lancet Global Health 9(4), 489-497.