Non-Specific Steroid Cell Tumor of The Ovary: Case Report And Review of The Literature
Abstract
Steroid cell tumors of the ovary are particularly rare, secreting sex hormones, characterized by steroid cell proliferation and represent only 0.1% of all ovarian tumors. They are classified into three subtypes according to their cell of origin: stromal luteoma, Leydig cell tumors and a third subtype of unknown lineage corresponds to a not specified steroid cell tumor (SCT-NOS). This third subtype accounts for 60% of steroid cell tumors. The clinical manifestations of SCT-NOS can take many forms, including pain, abdominal distension, but perhaps the most visible presentations are those related to hormonal activity and virilization of the tumor. We present a rare case of a 48-year-old woman with vaginal bleeding and a history of trunk obesity, hirsutism for 2 years and hypothyroidism with hormone replacement therapy. Clinical examination revealed a characteristic of obesity, virilization. Serum testosterone was 3.62 µg / L and CA-125 was 40.67. Magnetic resonance imaging identified a left ovarian solid mass and histopathology confirmed a steroid cell tumor not specific. The patient underwent exploratory laparotomy and left salpingoophorectomy. Macroscopically, the mass is well circumscribed, solid, homogeneous and yellowish. Microscopically, the tumor is mainly composed of eosinophilic or vacuolar granular cytoplasm. Immunohistochemistry showed that the tumor cells were strongly positive for inhibin. The postoperative period was uneventful. Through this rare observation, we will discuss the aspects that characterize this type of tumor and present some guidelines to be used in the differential diagnosis, as well as the difficulties encountered in the clinical, radiological and therapeutic fields.
Article Information
- Received
- Accepted
- Published
Academic Editor: Rongbiao Tang, Department of Radiology, Ruijin hospital, School of Medicine,
Checked for plagiarism: Yes
Review by: Single-blind
Copyright © 2022 M Darouichi
 This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Corresponding author: Corresponding author: M. Darouichi, Institute Medical Champel, 1206 Champel, Geneva, Switzerland —
Competing Interests
The authors have declared that no competing interests exist.
Funding
No specific funding statement was provided by the authors.
Data Availability
No data-availability statement was provided by the authors.
Acknowledgements
We thank Dr Aida Darouichi for professional advice and support during this study.
Citation:
Introduction
Steroid cell tumors of the ovary are particularly rare, accounting for 0.1% of all ovarian tumors. Steroid cell tumors a not otherwise specified (SCT-NOS) are a rarely subtype stromal tumors of the ovarian sex cord, which have a difficult clinical and radiological presentation. A few cases of SCT-NOS have been described in the literature. Appropriate evaluation is recommended for patients with symptoms of virilization such as hirsutism, amenorrhea, and ovarian mass. The histological, clinical, and radiological features of SCT-NOS are briefly summarized. A discussion of the differential pathologic, radiologic diagnostic criteria, guidelines, and treatment options appropriate for this tumor are presented in this article along with a review of the literature.
Case Report
A 48-year-old premenopausal woman in her 48th year had hair growth on her face and back over the past 2 years, bleeding from her vagina for 3 weeks and lower abdominal pain for 1 week. She had a history of recent weight gain, voice changes and medication use. There was a history of hypertension and hypothyroidism with hormone replacement therapy. There was no history of gynecological or breast tumors in the family. The examination revealed a patient with no objective clinical signs. Her BMI was 34.81 kg/m2 with a weight of 91 kg and a height of 167 cm. Systemic examination was normal. The patient was evaluated for bleeding and androgen excess characteristics. Pelvic ultrasound showed a normal uterus and a left ovarian mass of 5 cm. The DHEAS was 117 µg / dL and serum testosterone were elevated to 6.3 ng / mL (normal 0.1 - 1.2 ng / mL). CA-125 was 40.67 IU/mL, LH was 0.07 MIU/mL (normal 15.9-54 MIU/mL) and FSH was 0.37 MIU/mL (normal 23.0-116.3 MIU/mL). The dexamethasone suppression test suppressive cortisol by 19.29-0.81 µg/mL
Une IRM realized without and with contrast Gadolinium, in sequence T1,T2, DIFFUSION and confirmed one left masse ovarian
(Figure 1) , ( A, B) Axial T1-Weighted image shows (6 cm) ovoid hypointense masse (arrows) in left adnexal region. Ill- defined area of high signal intensity is noted, indicating lipid content. On T2-weighted image, masse (arrows) is heterogeneously hyperintense(C). After gadolinium administration, T1-weighted image shows tumor (arrows) is very intensely enhanced (D,E,F). F, diffusion image
A stepwise laparotomy was performed, peritoneal fluid was sent for cytological analysis. There was a 4x4 cm friable yellow mass on the left ovary (Figure 2). A left salpingo-oophorectomy was performed and sent for frozen section (Figure 2 ), which revealed a steroid cell tumor of a benign nature characterized by polygonal cells with abundant clear to vacuolar cytoplasm with no evidence of necrosis, hemorrhage or increased mitosis (Figure 3) The oil-red stain showed abundant lipid content in the cells, confirming the diagnosis of non-specific steroid tumor and there were no malignant cells in the peritoneal fluid. The postoperative period was uneventful, and she was discharged on Day 6. (Figure 2)
(Figure 2), Gross examination shows an ovary weighing 93 g, measuring 8.5 x 5.5 x 3.5 cm. The surface is smooth. On sectioning, a yellowish multinodular lesion measuring 8 x 5 x 3 cm is found, without necrosis. Lobulated mass of the ovary with yellow-orange cut surface.
Histology shows no necrosis or intra-tumor hemorrhage. Less than one mitosis for every 10 W.H.P.'s. Nuclear atypia is moderate.
Crystals of Reinke were not seen. The staining of Oil-red-O has revealed numerous intracellular lipid droplets. No mitotic figures were identified. No hemorrhagic or necrotic contents were noted.
(Figure 3), On immunostaining, tumor cells are positive for SF1, Calretinin and Inhibin. On the other hand, they are negative for Melan-A. 2, 10.
Figure 1A. Sequence T1 without contrast B) Sequence T2 without contrast c) T2 with contrast GADO D) Sequence T1 with contrast GADO E) Sequence T1 with contrast GADO F) Sequence diffusion
Download figure
Figure 2. Anatomopathological and Immunohistochemistry
Download figure
Figure 3. Photo HE et 4 IHC: 3 positives (inhibin, calretinin et SF1) et one negative (Melan A).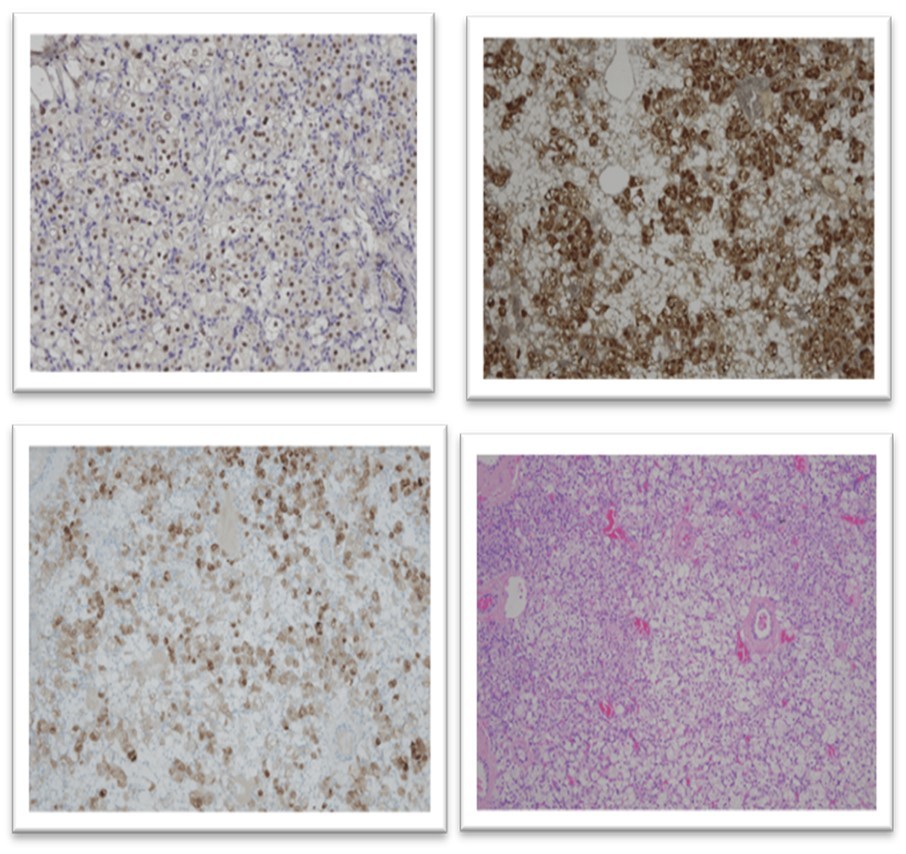
Download figure
Discussion
Ovarian steroid cell tumors are a rare tumor that secrete sex hormones and are characterized by a proliferation of steroid cells. They account for less than 0.1% of all ovarian tumors and are grouped into three subtypes according to their cells of origin: stromal luteoma, Leydig cell tumor (or hilus) and steroid cell tumor not otherwise specified (SCT-NOS) 2.
The first description and term of steroid cell tumor not otherwise specified was given in 1979 by Scully 1. SCT-NOS have a 60% incidence of ovarian steroid cell tumors. The English literature mentions less than a hundred cases through the PubMed search 3. It occurs at any age, with a high incidence between the third and fourth decade. To date, rare cases have been reported in the literature in children as young as 2 years of age and postmenopausal women 4.
They are mostly benign, diagnosed early at stage I at presentation with good prognosis, however malignant development with metastasis occurs in 25 to 40% of cases 5. SCT-NOS tumors are often unilateral in 94% of cases, although rare bilateral cases have been described in the literature 6.
This tumor produces several steroids, particularly testosterone, and are associated with androgen changes in 55-75% of cases 7. The main manifestation in 56-77% of patients is virilization with hirsutism, acne, voice changes, temporal baldness. Only 10% of patients suffer from amenorrhea 8. Manifestations such as hypothyroidism, endometrial hyperplasia or menorrhagia are associated in 6 to 23% of cases 9. Cushing's syndrome has been reported in 6-10% due to elevated plasma pro-renin and hypokalemia 10. Occasionally, HAT, stretch marks, hyper pilosis, osteoporosis, and acne are seen objectively.
However, 25% of patients with SCT- NOS, are asymptomatic, non-functional tumor 11, and their diagnosis is made postoperatively by immunohistochemistry.
To make a definite diagnosis of an endocrine tumor of ovarian origin, hormonal tests will be required. Elevated testosterone levels with normal levels of DHEA, LH, FSH and 17-hydroxyprogesterone are indicative of a virilizing tumor of the ovary.
There are three main markers of ovarian cancer: CA 125, CA 19-9 and ACE 12. Only CA 125 is of primary importance since its rate is increased regardless of histological type 13. According to Malkasaian et al 14, a CA125 level greater than 65 µ/ml is predictive of malignancy in 98% of cases, while a low level is predictive of benignity in 72% of cases. However, CA125 levels may increase in other cancers (cervix, endometrium, digestive tract). In Hayes and Scully's studies, five pathological signs are linked to the malignancy of these tumors, namely more than two mitoses, necrosis, a diameter greater than 7 cm, hemorrhagic foci and nuclear atypia of two or three. 15.
MR imaging and color flow Doppler ultrasound are two excellent imaging modalities that may demonstrate characteristic radiologic features and characterization differential diagnosis for these tumors.
Sonography is generally used as the first-line imaging technique for the evaluation of ovarian pathologic abnormalities. It makes it possible to specify the tumor ovarian origin; its structure, dimensions, solid and/or cystic component, its vascularization, either unitary or bilateral, also show its extension to adjacent organs. The SCT-NOS ovarian tumor varies in size from 1.5 cm to 40 cm and is bilateral in 6% of cases 16. Ultrasound remains effective in postmenopausal women with atrophied ovaries and less accurate in younger women.
MR imaging is useful for identifying these tumors in young and postmenopausal women 17. The diagnosis of an ovarian tumor is made by clearly indicating its location, size, contour and the presence or absence of an adjacent or distant malignant abnormality. This technique allows optimal exploration in all 3 planes as well as the characteristics of the diffusion and perfusion of the lesion and the pattern of enhancement (homogeneous or heterogeneous) after gadolinium injection.
Laparoscopy is indicated when the ultrasound scan is not formal and when there is doubt about the organic nature of the lesion. It eliminates non-ovarian lesions, determines the ovarian tumor and makes an etiological diagnosis by cytological punctures of the mass.
Macroscopically, these tumors are typically very limited, well circumscribed and unilateral, yellow to orange, red or brown in color depending on the lipid content. It varies in size from 1 cm to 45 cm, with a generally solid consistency, but a combination of solid and cystic forms can be observed. In our case, the tumor was entirely solid, with no cystic area. Its cross-sectional area was generally yellow and lobulated 18.
Histological examination allows the definitive diagnosis and is confirmed by immunohistochemistry. Cells with abundant granular or vacuolar eosinophilic cytoplasm, positive for fat spots and negative for Reinke's crystals and stromal hyperthecosis were found 19. Immunohistochemical validation is necessary condition for the definitive diagnosis of SCT-NOS. Inhibin is positive in most steroid cell tumors and is very useful in the differential diagnosis between sex cord tumors and non-steroid cell tumors. These tumors are negative for CK and EMA, although a small subset of tumors may be positive for EMA. This presentation diagnosed SCT-NOS based on microscopic images and found that our case had positive immune reactivity: 3 positive (inhibin, calretinin and SF1) and negative (Melan A) 20.
SCT-NOS steroid cell tumors should be differentiated from other types of steroid cell tumors, in which the development of steroid hormone-producing cells occurs secondarily.
This includes granulosa cell tumors, fibroids and thecomas, stromal luteoma and Leydig cell tumor.
1) Granulosa cell tumors are the most common malignant stromal tumors and are often revealed at stage 1 at diagnosis. They constitute the main group of hormone-secreting ovarian tumors and are subdivided into two different clinicopathological subtypes: adult and juvenile, depending on age, and are distinguished by size and solid or cystic type 21. The adult form occurs in women over 30 years of age and postmenopausal. As for the juvenile subtype, it appears mainly in children. These tumors are easier to diagnose because of their characteristics, since they have a differentiated radiological and histological behavior 22. In terms of imaging, these tumors are very diverse, ranging from solid masses through hemorrhagic or fibrous tumors to multilocular or simply cystic lesions 23 (Table 1). An assessment of the underlying histopathological parameters of the tumor is essential for a definitive diagnosis. In adults, these tumors are characterized by pale nucleus tumor cells, often with regular mucin-depleted follicles, longitudinal grooves and an emergency corpus callosum 24. Whereas in the juvenile type, dark nuclei with irregular follicles contain mucin and are only rarely striated or have the microfollicular pattern, with numerous rosette-like structures that simulate the Call-Exner bodies of the Graafian follicle 25. Recently, a mutation of the FOXL2 gene has been detected in the majority of adult granulosa cell tumors (97%), and very rarely in juvenile tumors (10%) 26. The distinction between AGT and undifferentiated carcinomas, the positive immunostaining test for α-inhibin, calretinin and vimentin, and the lack of staining for EMA all argue in favour of a diagnosis of AGT. A FOXL2 immune reaction is useful 27. The prognosis varies according to the stage of diagnosis, tumor size and nuclear atypia. Survival at 10 years is greater than 90% with local recurrence and a 5-25% risk of malignancy at 20 years 28.
2) Fibroma, fibro-thecomas and thecomas are benign ovarian tumors, accounting for 4%-6% of all ovarian tumors and affect pre- and post-menopausal women. Thecomas are stromal tumors composed of theca-type lipids, as well as lutein cells and fibroblasts 29. They occur in elderly patients with estrogenic activity and are associated with uterine bleeding, with 21% having endometrial carcinoma 30. They are unilateral in 97% of cases and consist of round to spindle-shaped cell sheets with an ill-defined pale cytoplasm, usually vacuolated and lipid-rich, and alternating with collagen-producing fibroblasts. Thecomas are immunoreactive to vimentin, inhibin, calretinin and other sex cord markers 31. Radiologically, they are usually solid masses with T2-weighted dark MRI signal intensity and a variable rate of calcification or degeneration 32. Thecomas typically are usually benign and surgical excision is the best treatment 33.
Fibromas are composed of a non-functional stroma with no estrogenic activity, formed exclusively of collagen-producing spindle cells containing only small amounts of cytoplasmic lipids 34. In CT Scanner, they appear as a homogeneous solid tumor, with delayed contrast on I.V. and MRI, a T1-weighted iso intense mass and a T2-weighted hypointense mass. Hypointense calcifications and hyperintense areas, occasionally scattered, were often observed, indicating edema or a cystic degeneration 35. Lastly, fibroids containing ≥ 4 mitoses per 10 HPF are now known as "mitotically active cellular fibroids" and should be distinguished from fibrosarcoma’s 36.
3) Sclerosing stromal tumors (SSTs) were first described by Chalvardijaian and Scully in 1973 37. They affect young women with menstrual disorders and lower abdominal mass. However, SSDs remain very limited and are devoid of Reinke's crystalloids 38. They are characterized by cellular areas separated from each other by hypocellular areas composed of dense collagen, edematous or myxoid tissues and by significant vascularization, all forming a pseudo-lobular structure 39. The cytoplasm is moderately abundant, eosinophilic and sometimes vacuolized 40. On non-contrast CT, SST shows solid densities corresponding to cellularity, vascularity, and distribution of collagen or fibrous stroma, while foci of necrosis or cystic degeneration are low density 41. In the arterial phase, after intravenous administration of contrast material, rapid improvement of the external region of the tumor is observed due to the cellular area with numerous vascular spaces. In the venous phase, an extension of the reinforcement zone is observed on the internal part of the lesions in association with a hypocellular collagen zone. The areas of the tumor that do not show obvious improvement correspond to the edematous regions. On MRI, they appear as a large mass with hyperintense or heterogeneous solid cystic components, iso to hyperintense in T2-weighted sequence. They are slow-growing tumors with a hypo-intense peripheral edge in T2 and a thin ovarian cortex 42. Following injection of gadolinium, the intense and early contrast of the septum between internal and peripheral cysts with centripetal progression reveals hypercellularity with an abundant vascular network. The differential diagnosis of TSS should also include other thecoma-fibroma and malignancies 43, because of its rarity, since diagnosis by prospective imaging is not possible. Surgical resection of the tumor is curative and local or distant recurrence should be avoided.
4) Sertoli-Leydig cell tumors are very rare and benign and occur in young women with clinical androgenic symptoms and account for less than 0.5% of ovarian tumors 44. These tumors are almost always unilateral and are either solid and cystic or papillary. They appear as a well-defined solid mass with intra-tumoral cysts on CT scan and hypo-intense cysts with numerous cystic areas of varying size on MRI 45. They are also known as androblastomas and are the most common virilizing tumors 46. They secrete androgens with male characteristics such as amenorrhea, facial hair, low voice, chloritoid hypertrophy and hyper seborrhea 46. Leydig cells are classified by Roth and Steinberg into two basic forms 47:
the dominant hilar form, consisting of a small benign unilateral nodule. Leydig cells are well limited with Reinke's crystalloids in 50% of cases 48.
the non-hilar form consists of tumors of the ovarian stroma, located in the ovarian parenchyma and containing 100% Reinke's crystalloids.
Anatomopathological, they are small reddish-brown lesions with eosinophilic cells with low cytoplasmic lipid content, presenting mainly intracytoplasmic Reinke crystals. Their nuclei are hyperchromatic and have only one small nucleolus. Mitoses are rare and always benign 49. On MRI, a small mass with hyper-intense areas can be seen on sequqncesT1-weighted images due to the abundance of intracellular lipids and the large increase in contrast medium after gadolinium injection due to rich vascularity 50.
Treatment
The basic therapy for steroid-induced ovarian tumors is total abdominal hysterectomy with bilateral salpingo-oophorectomy and complete surgical staging. However, for women who wish to maintain their fertility, conservative surgical treatment with unilateral oophorectomy may be accepted.
Surgical management of SCT-NOS should be prompt, imperative, based on two essential elements: histological type and patient desires.
In the first instance, satisfactory resection of the tumor must be carried out for any benign or malignant case with multiple variants 51:
-Total hysterectomy with bilateral salpingectomy for elderly women who do not wish to preserve the uterus.
For young women, before the age of 40, conservative treatment is applied in the case of benign tumors, with a conservative cystectomy to preserve ovarian function.
Uni-lateral salpingo-ovarectomy in women of child-bearing age with a benign tumor.
Unilateral salpingo-ovarectomy with malignant tumor and preservation of the uterus for future fertility, but close monitoring with staging is essential.
Metastatic malignant tumour, requires post-operative adjuvant chemotherapy BEP, Bleomycin, Etoposide and Cisplatin. The best adjuvant chemotherapy is still unknown 52.
In our case, the patient is young and eager to have children, and has had a successful unilateral sapling-oophorectomy.
Prognosis
For this, it is important to establish a close correlation between various clinical, pathological parameters and the undesirable behavior of the tumor, such as the age of patients in the clinical stage, tumor size greater than 7, 0 cm or more (78% malignant tumors), pituitary field mitoses greater than 2 mitoses (92% malignant tumors), grade 2-3 nuclear atypia (64% malignant tumors), necrosis (86% malignant tumors) and hemorrhage (77% malignant tumors) 53.
Regular monitoring with measurement of serum testosterone levels is mandatory, and since little is known about the behavior of these tumors, it is not known for how long.
In our case, the prognosis is favorable since the size of the tumor is less than 7 cm, without mitosis, necrosis or hemorrhage. Clinically malignant tumours occur in 25 to 43% of cases, whereas clinically malignant cases are histologically benign 53.
Table 1. Typical Appearances of More Common Sex Cord-Stromal Tumors| S. No | Tumor | Typical Tumor Morphology | Key Imaging Features |
| 1 | GCT | ||
| Juvenile | Multicyclic | Hemorrhage, pseudoprecocious puberty | |
| Adult (polyps, earcinoma) | Solid or multicystic and solid | Hemorrhage, spongelike cysts in tumor, endometrial abnormalities | |
| 2 | The coma | Solid | Nonspecific |
| 3 | Fibroma | Solid | Sound attenuation at US, low signal at T2 weighted MR imaging |
| 4 | Sertoli-Leydig tumor | Solid | Nonspecific |
| 5 | Steroid cell tumor | Solid | Nonspecific |
Conclusion
SCT-NOS are particularly rare stromal tumors of the ovarian sex cord, which are difficult and misleading to diagnose clinically and radiologically, as this observation demonstrates. For early diagnosis, careful physical examination, supplemented by laboratory values and imaging, is useful in patients with symptoms of virilization and amenorrhea. In most cases, typical histopathological analyses confirm the diagnosis. In case of difficulties, immunohistochemistry is an important diagnostic tool. Treatment depends on the histology, surgical stage and the desire to preserve fertility. The treatment of malignant tumors should combine surgery and chemotherapy.
References
- 1.Scully R E. (1979) Tumors of the ovary and maldeveloped gonads. Atlas of tumor pathology, fasc 16, ser 2. Washington, DC: Armed Forces Institute of Pathology In: Hartmann WH, ed .
- 2.Singh P, Deleon F, Anderson R. (2012) Steroid cell ovarian neoplasm, not otherwise specified: a case report and review of the literature. Case Rep Obstet Gynecol.:. 2531522012.
- 3.Young R H, Scully R E. (1994) Sex cord-stromal, steroid cell, and other ovarian tumors with endocrine, paraendocrine, and paraneoplastic manifestations. Blaustein’s pathology ofthe female genital tract. 4th ed In: Kurman RJ, ed , New York, NY: 783-847.
- 5.Hayes M C, Scully R E. (1987) Ovarian steroid cell tumors (not otherwise specified): a clinicopathological analysis of 63 cases. , Am J Surg Pathol; 1, 835-845.
- 6.Azizlerli H, Tanakol R, Terzioglu T. (1997) Steroid cell tumor of the ovary as a rare cause of virilization. , Mt Sinai J Med 64, 130-5.
- 7.Mizoguchi M, Minami S, Yamamoto M, Tanizaki Y, Kobayashi A et al. (2014) Ovarian steroid cell tumor, not otherwise specified, producing testosterone. , Journal of Obstetrics and 40(9), 2081-2085.
- 8.Qian L, Shen Z, Zhang X, Wu D, Zhou Y. (2016) Ovarian steroid cell tumor, not otherwise specified: a case report and literature review. Molecular and Clinical Oncology.;5(6):. 839-841.
- 9.Tsai H J, Chen S C, Wei H Y. (2007) Hypothyroidism and hyperlipidemia with a virilizing ovarian steroid cell tumor, not otherwise specified. , Gynecol Endocrinol; 23, 69-71.
- 10.Donovan J T, Otis C N, Powell J L. (1993) Cushing’s syndrome secondary to malignant lipoid cell tumor of the ovary. , Gynecol Oncol; 50, 249-53.
- 11.Das A, Panda S, A S Singh. (2015) Steroid cell tumor: a rare virilizing ovarian tumor,”. , Journal of Cancer Research and Therapeutics 11(3), 660.
- 12.H Schieder Koelbl, Neunteufel K, Bieglmayer W. (1989) C A comparative study of mucin-like carcinoma-associated antigen (MCA). , CA 125, CA 36(4), 473-478.
- 13.M Yumru Bozkurt, Aral A E. (2013) I Evaluation of the importance of the serum levels of CA-125, CA15-3, CA-19-9, carcinoembryonic antigen and alpha fetoprotein for distinguishing benign and malignant adnexal masses and contribution of different test combinations to diagnostic accuracy. , Eur J Gynaecol Oncol ; 34(6), 540-544.
- 14.GD Knapp Malkasian, Lavin R C, PT. (1988) Preoperative evaluation of serum CA 125 levels in premenopausal and postmenopausal patients with pelvic masses: discrimination of benign from malignant disease. , Am J Obstet 159(2), 341-346.
- 16.Atri M, Nazarnia S, Bret P M, Aldis A E, Kintzen G et al. (1994) Endovaginal sonographic appearance of benign ovarian masses. , RadioGraphies; 14, 747-760.
- 17.Wang P H, Chao H T, Lee R C. (1998) Steroid cell tumors of the ovary: clinical, ultrasonic, and MRI diagnosis-a case report. , EurJ Radiol; 26, 269-273.
- 18.Rabban J T, Zaloudek C J. (2013) A practical approach to immunohistochemical diagnosis of ovarian germ cell tumors and sex cord-stromal tumors. , Histopathology 62, 71-88.
- 19.Zhao C, Vinh T N, McManus K, Dabbs D, Barner R et al. (2009) Identification of the most sensitive and robust immunohistochemical markers in different categories of ovarian sex cord-stromal tumors. , Am J Surg Pathol 33, 354-366.
- 20.Movahedi-Lankarani S. (2002) Calretinin, a more sensitive but less specific marker than alpha-inhibin for ovarian sex cord-stromal neoplasms: an immunohistochemical study of 215 cases. , Am J Surg Pathol.. PMID: 12409724.
- 21.StenwigJT HazekampJT, BeechamJB. (1979) Granulosa cell tumors of the ovary: a clinicopathological study of 1 18 cases with long-term follow-up. , Gynecol Oncol; 7, 136-152.
- 22.Young R H, Dickersin G R, Scully R E. (1984) Juvenile granulosa cell tumor of the ovary. A clinicopathologic analysis of 125 cases. , Am J Surg Pathol 8, 575.
- 23.Kim S H, Kim S H. (2002) Granulosa cell tumor of the ovary: common findings and unusual appearances on CT and MR. , J Comput Assist Tomogr; 26, 756-761.
- 24.Gusberg S B, Kardon P. (1971) Proliferative endometrial response to theca granulosa cell tumors. , Am J Obstet Gynecol 111, 633.
- 25.Nakashima N, Young R H, Scully R E. (1984) Androgenic granu1osa cell tumors of the ovary. A clinicopathologic analysis of 17 cases and review of the literature. , Arch Pathol Lab Med 108, 786.
- 26.R J Kurman. (2014) International Agency for Research on Cancer, and World Health Organization, WHO classification of tumours of female reproductive organs. International Agency for Research on Cancer, Lyon, 4th .
- 27.Troiano R N, Lazzarini K M, Scoutt L M, Lange R C, Flynn S D et al. (1997) Fibroma and fibrothecoma of the ovary: MR imaging findings. , Radiology; 204, 795-798.
- 28.Bjorkholm E, Silfversward C. (1981) Prognostic factors in granulosa cell tumors. , Gynecol Oncol 11, 261.
- 30.H Burandt E Young R. (2014) Thecoma of the ovary: a report of 70 cases emphasizing aspects of its histopathology different from those often portrayed and its differential diagnosis.Am. , J Surg Pathol.; 38, 1023-1032.
- 31.Torricelli P, Caruso Lombardi A, Boselli F, Rossi G. (2002) Sclerosing stromal tumor of the ovary: US, CT and MRI findings. , Abdom Imaging; 27, 588-591.
- 32.Kim I, Young R H, Scully R E. (1985) Leydig cell tumors of the testis. A clinicopathological analysis of 40 cases and review of the literature. , Am J Surg Pathol.; 9, 177-92.
- 33.Weinreb J C, Barkoff N D, Megibow A, Demopoulos R. (1990) The value of MR imaging in distinguishing leiomyomas from other solid pelvic masses when sonography is indeterminate. , AJR; 154, 295-299.
- 34.Talerman A. (1989) Ovarian sertoli-leidg cell tumor (androblastoma) with retiform pattern : aclinico-pathologic study.Cancer.;60:. 3056-64.
- 35.Dockerty M B, Masson J C. (1944) Ovarian fibromas: A clinical and pathologic study of two hundred and eighty-three cases. , Am J Obstet Gynéco 47, 741.
- 36.H Irving J A Alkushi A Young R. (2006) Clement P.B. Cellular fibromas of the ovary: a study of 75 cases including 40 mitotically active tumors emphasizing their distinction from fibrosarcoma. , Am J Surg Pathol.; 30, 928-938.
- 37.H Bennett J A Oliva E Young R. (2015) Sclerosing stromal tumors with prominent luteinization during pregnancy: a report of 8 cases emphasizing diagnostic problems.Int. , J Gynecol Pathol.; 34, 357-362.
- 38.H Staats P N McCluggage W G Clement P B Young R. (2008) Luteinized thecomas (thecomatosis) of the type typically associated with sclerosing peritonitis: a clinical, histopathologic, and immunohistochemical analysis of 27 cases. , Am J Surg Pathol.; 32, 1273-1290.
- 40.Gershenson D M. (1994) Management of early ovarian cancer: germ cell and sex cord-stromal tumors. Gynecol Oneol;. 55-62.
- 41.Ann G H, Lee SK ChiJG. (1986) Ovarian sex cord tumor with annular tubules. , Cancer; 57, 1066-1073.
- 42.Young R H, Welch W R, Dickersin G R, Scully R E. (1982) Ovarian sex cord tumor with annular tubules: review of 74 cases including 27 with Peutz-Jeghers syndrome and four with adenoma malignum of the cervix. , Cancer; 50, 1384-1402.
- 43.Tsuruchi N, Tsukamoto N, Kaku. (1994) Adenoma malignum of the uterine cervix detected by imaging methods in a patient with Peutz-Jeghers syndrome. , Gynecol Oncol 1, 232-236.
- 44.Young R H, Scully R E. (1985) Sertoli-Leydig cell tumors: A clinicopathological analysis of 207 cases. , Am J Surg Pathol 9, 543.
- 45.Baiocchi G, Manci N, Angeletti G, Celleno R, Fratini D et al. (1997) Pure Leydig cell tumour (hilus cell) of the ovary: a rare cause of virihization after menopause. , Gynecol Obstet Invest; 44, 1144.
- 46.Young R H, Scully R E. (1984) Well differentiated ovarian Sertoli-Leydig cell tumors. A clinicopathological analysis of 23 cases. , Int J Gynecology Pathol 3, 277.
- 47.Yanushpolsky E H, Brown D L, Smith B L. (1995) Localization of small ovarian Sertoli-Leydig cell tumors by transvaginal sonography with color Doppler. Ultrasound Obstet Gyneeol;. 5, 133-135.
- 48.Moltz L, Pickartz H, Sorensen R, Schwartz U, HammersteinJ. (1983) A Sertohi-Leydig cell tumor and pregnancy: clinical, endocrine, radiology, and electron microscopic findings. , Arch Gynecol; 233, 295-308.
- 49.Young R H, Scully R E. (1983) Ovarian Sertoli-Leydig cell tumors with a retiform pattern: A problem in histopathologic diagnosis. , Am J Surg Pathol 7, 755.
- 50.Young R H, Dudley A G, Scully R E. (1984) Granulosa cell, Sertoli-Leydig cell and unclassified sex cord-stromal tumors associated with pregnancy: A clinicopathologic analysis of thirty-six cases. , Gynecol Oncol 18, 181.
- 51.Wang P-H, Chao H-T, Lee R-C. (1998) Steroid cell tumors of the ovary: clinical, ultrasonic, and MRI diagnosis—a case report,”. , European Journal of 26(3), 69-273.