
Abstract
Background
Pregnancy and parturition are events of considerable significance in the life cycle of women. Though it is supposed that the quality of care during labor, birth, and postpartum period plays a great role for adverse outcomes of birth, various reports claimed that cesarean delivery carries a higher maternal and fetal morbidity and mortality compared to vaginal delivery. Therefore, this study assessed the Rate, Maternal and Fetal Outcome of Cesarean delivery performed by IESO at Shenen Gibe General Hospital, Jimma south west Ethiopia. Integrated Emergency surgical officer is a health professional qualified and authorized to perform emergency obstetrical-gynecological and emergency general surgical procedures. The training has started in 2010 in 3 universities and 10 affiliated sites with intake of 43 students. The MSc program in integrated emergency surgery is intended to achieve one of the millennium development goals (MDG): reducing the overwhelming maternal mortality ratio and perinatal mortality rate at the local and national level. (1)
Methods
Hospital based two-year retrospective descriptive cross-sectional study design was employed and data collected from November to December 2019 in shenen Gibe General Hospital ,Jimma south west Ethiopia. A total of 185 mothers who delivered by cesarean delivery from December 2017 to December 2018 and complete data were included in the study. Data were extracted using structured data collection format and cleaned, and entered into Epi data software version 3.1 and exported into SPSS version 26 for further descriptive analysis.
Result
Among 2115 deliveries in the two years of retrospective data, a total of 186 mothers were delivered by cesarean section, giving cesarean delivery rate 8.8 %. The leading indication for cesarean delivery was fetal distress (24.2%). Among the total cesarean delivery, 22 neonates were died, giving the proportion of neonate mortality rate 16.8%. One mothers were died following cesarean delivery, giving maternal mortality rate following cesarean delivery 12 per 1000 live births. The leading cause for maternal mortality was hemorrhagic shock
Conclusion
However, cesarean delivery rate in this study was within the WHO recommended range, the health outcome of mothers and neonates’ following cesarean delivery was not acceptable. The neonatal and maternal mortality following cesarean delivery was 16.8% and12 per 1000 live births respectively. The main cause of neonatal death was birth asphyxia.
Author Contributions
Academic Editor: AnnamariaZsakai, Eotvos Lorand Universit, Hungary.
Checked for plagiarism: Yes
Review by: Single-blind
Copyright © 2020 Worku Gebeyehu Gutema, et al.
 This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Competing interests
The authors have declared that no competing interests exist.
Citation:
Background
Basic obstetric and newborn care provided by skilled attendants during prenatal and delivery has good maternal and neonatal outcomes 1, 2. Cesarean delivery as one of life saving procedure has played a major role in lowering both maternal and neonatal mortality rate 3. Cesarean delivery refers to the delivery of a fetus, placenta and membrane through the abdominal and uterine incision after 28 weeks of gestation 4. Though cesarean delivery is considered as a life-saving intervention for both the maternal and a child health, the quality of obstetric care further determines the outcomes of the mother as well as the fetus 5, 6, 7. Cesarean delivery unless used appropriately, the potential risk to the mother and baby becomes more than the vaginal delivery, therefore it can considered as the vital indications of the health status of the neonate and the mother 6, 8, 9, 10.
Poor outcomes of cesarean delivery among mothers and fetus in developed and developing countries were reported consistently higher compared to vaginal deliveries 3, 11, 12. In resource-poor countries where poor quality of obstetric care is the problem, and most cesarean deliveries are performed when a vaginal delivery puts the babies or the mother’s life or health at risk, cesarean delivery is the marker for poor outcomes of maternal and neonatal health 1, 3, 11, 13. Unlike developed countries, most cesarean deliveries in developing countries are conducted because of obstetrical complications or medical illness. Consequently, the risk of cesarean delivery may be worsening if it is performed under emergency situations 14, 15, 16.
Though, World Health Organization suggesting that cesarean rate should not exceed 15% 17, 18, rate of cesarean delivery are increasing dramatically. Due to the rising CS rate in both developed and developing countries, mothers and neonates are also vulnerable to unnecessary risks. However, there is variation on the rate of cesarean delivery in the world; rate of cesarean delivery in developed nations ranged from 12 to 86% 8, 19, 20, 21. In developing countries, especially in Sub-Saharan country where maternal and neonatal mortality rate is high, maternal and infant mortality corresponding with the increasing rate of cesarean delivery is associated with the quality of obstetric service during pregnancy and childbirth. In low and middle income countries, the rate of cesarean delivery range between 2 to 39% 18, 19, 22, 23
Maternal and neonatal morbidity and mortality is not only accounted by the surgical procedure, but also other risk factors such as un-booked status, severe blood loss 11, 12, 24, 25, previous antenatal care service, use of general anesthesia, anemia, dehydration, prolong labor, repeated vaginal examination, previous surgery Gestational age, and medical condition diagnosed before cesarean section and scarcity of senior obstetricians 26, 27, 28, 29.
Emergency surgical officer is a health professional qualified and authorized to perform emergency obstetrical-gynecological and emergency general surgical procedures. The training has started in 2010 in 3 universities and 10 affiliated sites with intake of 43 students. The MSc program in integrated emergency surgery is intended to achieve one of the millennium development goals (MDG): reducing the overwhelming maternal mortality ratio and perinatal mortality rate at the local and national level. (1) Ethiopia is well-known by high maternal, perinatal and infant mortality rates and trauma relate morbidity and mortality. Therefore, reduction of the morbidities and deaths in our country will require a shift in the strategy that will ensure that majority of emergencies and births are attended by appropriately trained and skilled healthcare professionals including nurses, midwives, health officers and doctors able to prevent, detect and manage obstetric complications and surgical emergencies. (2)
The IESO program is thus developed to produce emergency surgical officers in Ethiopia capable to handle common emergency obstetrical gynecological and emergency general surgical procedures including trauma at accessible locality. After a 3 years intensive training on integrated emergency surgery, a surgical officer is expected to undertake the following activities and procedures. Diagnose common general surgical and obstetrical emergency problems, make a sound decision in clinical management, perform emergency vaginal surgical procedures if indicated, e.g. Vacuum extraction and craniotomy, Perform emergency caesarean section, emergency hysterectomy, and laparotomy for tubal pregnancy, Perform appendectomy, emergency small bowel resection and anastomosis, repair bowel perforation, colostomy, cystostomy and abscess drainage ,Handle emergency trauma including fracture, dislocation, amputation, debridement, and septic arthritis, Manage intraoperative and postoperative complications, competent in cardiorespiratory resuscitation, primary care of head injuries, and thoracostomy, Diagnose and manage common emergency medical problems(2)
Reducing maternal mortality and providing universal access to reproductive health in resource limited settings has been severely constrained by a shortage of health workers required to deliver evidence based interventions(3). Task shifting has been highlighted as an important strategy to optimize health worker performance in resource poor settings (PMNCH/ WHO 2010) and provide the right mix of skills required to undertake the activities required for the service. (4)
The delegation of maternal and reproductive health care duties to other cadres is practiced in many countries(5). One such group has been labelled ‘mid-level’ cadres and includes non-physician clinicians (NPC), nurses, midwives, auxiliary nurses and midwives and community health workers (CHWs). Despite the 2009
Based on a study by Dawson et al, on task shifting and sharing in maternal and reproductive health in low-income countries which focuses on clinical tasks (the delivery of obstetric surgery, anesthesia and abortion) that were shifted to and/or shared with doctors, non-physician clinicians, nurses and midwives concluded that shifting and sharing these tasks may increase access to and availability of maternal and reproductive health services without compromising performance or patient outcomes and may be cost effective (7)
In Ethiopia, maternal and neonatal morbidity and mortality rate is high. Maternal and neonatal death in the country is reported as 470 per 100,000 live birth and 37 per live births respectively. Though, institutional delivery rate across the country become increasing, the change in reducing maternal and neonatal mortality rate is not reduced substantially. According to 2011 Ethiopian demographic and health survey report, 2% of the pregnant women are delivered with cesarean section which is increased by 1% from the 2010 Demographic and health survey report 30, 31, 32. Therefore, this study assessed Rate, Maternal and Fetal Outcome of Cesarean delivery performed by Integrated emergency surgical officers at Shenen Gibe General Hospital, Jimma south west Ethiopia.
Methods and Materials
Study Setting
The study was conducted at Shenen gibe General hospital located in jimma town, Jimma is 335km from capital city of Addis. The service has been operating since 2012. The hospital provides health services for more than 500,000 residents of in the catchment areas at outpatient and inpatient wards. The hospital provides inpatient service with 80 beds, and 6 delivery couches. Maternity and gynecologic services are the main surgical procedure done. Elective and emergency surgical services are performed. There are three integrated emergency surgical professional specialist , one internal medicine specialist ,two general Surgeon, nineteen General practitioner, eighteen midwives, forty four nurses, 7 lab technicians, two x-ray technician, one psychiatric nurses, one Doctor of dental, two optometrist, two health officers and eighty eight administrative staffs .
Study Design
Hospital based cross-sectional retrospective study was conducted from September 2017 to December 2018 at Shenen Gibe General hospital. A total 2,115 mothers are delivered during the period from September 2017 to December 2018 and 185 women were delivered by cesarean section.
Inclusion Criteria
All cesarean section performed after period of viability (28 weeks) including elective, emergency, primary and repeat cases are included in the study
Study Participants, Sample Size and Sampling Procedure
All women who delivered by caesarean section including a failed instrumental delivery between September 2017 to December 2018 at Shenen Gibe General hospital were the population under the study. All caesarean deliveries including elective, emergency, primary and repeat cases are included in the study. The charts of all 185 mothers who gave birth by caesarean section during the retrospective period were reviewed. Charts with incomplete information were excluded from the study.
Data Collection Tool and Procedure
Data were collected using pre-tested structured questionnaire using chart review method. The questionnaire consists of socio-demographic variables, obstetric history and outcomes of cesarean section. Mothers’ information including age, parity, gestational age, antenatal care, stage of labor at admission, fetal condition at admission, and onset of labor, (spontaneous or induced). Information was obtained from operation theatre, labor ward and neonatal ward records. The questionnaire was prepared in English. Three BSc midwifery as data collector and one general practitioners as supervisors were recruited for the study. Two days intensive training regarding the objective of the study, confidentiality of information, and techniques to conduct interview was given to data collectors and supervisors. To address the ethical issues, the data collectors were recruited among the permanent employees of the respective hospitals. Maternal death was defined as death of the mother during hospitalization. Early neonatal death was defined as death of the infant within 7 days of delivery. Cesarean section rates were calculated by dividing the total number of Cesarean section by the total number of deliveries excluding stillbirths.
Data Processing and Analysis
Data were entered into Epi-data version 3.1 and exported to SPSS version 26 for further analysis. Data cleaning was done by running frequencies. Descriptive statistics, including frequency and proportions were computed to summarize the study variables. Bivariate analysis and chi-square test were used to examine association between dependent and independent variable. A 95 % CI and P-value of <0.05 were considered to be statistically significant. In addition crude/Adjusted odd ratio were calculated. To assess the effect of each independent variable on the outcome variables multivariate logistic analysis was carried out and fit to the final model.
Result
Socio-demographic Characteristics of Respondents
From September 2013 to December 2015, there was a total of 2115 deliveries and 186 pregnant women delivered by a cesarean section giving an overall cesarean section rate 8.8 %. The proportion of cesarean section delivery was higher among rural residents, which was 75.3 %. A majority of cesarean section deliveries (61.3%) were in the age between 19 and 29 years of age. The mean (+SD) age of pregnant women who undergo cesarean section delivery was 27.85 years (+6.5). Nearly two third (73.6%) of mothers conduct the cesarean section delivery procedure were multiparous, while one hundred forty four (77.4%) mothers had antenatal care service register or they were booked and 32.8 percent of those underwent for cesarean delivery were had more than two visit. Around one hundred six (57.0%) of mothers were on active first stage of labor on admission. Sixty nine (37.1%) of mothers were had previous CS delivery. Among the total mothers who underwent cesarean delivery, majority (71.5%) of these women had emergency CS, and the higher (75%) of referred cases were responsible for majority of emergency CS. More than half (83.9%) of CS were made by spinal anesthesia and the remaining were general anesthesia (Table 1).
Table 1. Socio-demographic characteristics of respondents| S.no | variable | frequency | percent | |
| 1 | <18 | 8 | 4.3 | |
| 19-29 | 108 | 58.1 | ||
| 30-39 | 60 | 32.3 | ||
| >40 | 10 | 5.4 | ||
| 2 | Residency | urban | 46 | 24.7 |
| rural | 140 | 75.3 | ||
| 3 | ANC booking status | Yes | 144 | 77.4 |
| No | 42 | 22.6 | ||
| 4 | parity | Primi | 49 | 26.3 |
| Parous (2-4) | 81 | 43.5 | ||
| Grand multi >5 | 56 | 30.1 | ||
| 5 | GA | preterm | 14 | 7.5 |
| term | 168 | 90.3 | ||
| post term | 4 | 2.2 | ||
| 6 | Partograph | Yes | 126 | 67.7 |
| No | 60 | 32.3 | ||
Cesarean Section Rate, Maternal and Neonatal Outcomes of Cesarean Section (CS)
Among 2115 deliveries in the two years of retrospective data (from September 2013 to December 2015), a total of 186 mothers were delivered by cesarean section, giving cesarean section rate 8.8 %. Among the total deliveries (2115), one hundred thirty one (131) neonate and two (2) mothers were died, giving the overall neonatal and maternal mortality rate of the hospital as 61.9 per 1000 live births and 0.9 per 100, 000 live births respectively. while, among the total mothers who delivered by cesarean section (186), one mothers and 22 neonates were died, giving the proportion of maternal mortality rate and neonatal mortality rate following cesarean section 12 per 1000 live births and 16.8% were attributed due to cesarean section delivery. Respiratory failure was the major responsible causes of maternal deaths. Of the total mothers who conduct CS procedure; the leading indications of admission for cesarean section delivery were fetal distress (43%), scar plus premature rupture of membrane (29%) ante partum hemorrhage (23%) failed induction and augmentation (20%) Cephalo-pelvic disproportion (CPD) (19%), and fetal mal-presentation (18%). Figure 1.
Figure 1.Major Indication of Cesarean section (CS) in Shenen Gibe general Hospital, Southwest Ethiopia, 2020
From 186 mothers underwent Cesarean delivery 9.1 % would develop one or more complication, the most causes for these complications were puerperal sepsis, PPH, wound infection and anesthesia complication (Figure 2).
Figure 2.Causes of Maternal complication after Cesarean section in Shenen Gibe General Hospital, south west Ethiopia, 2020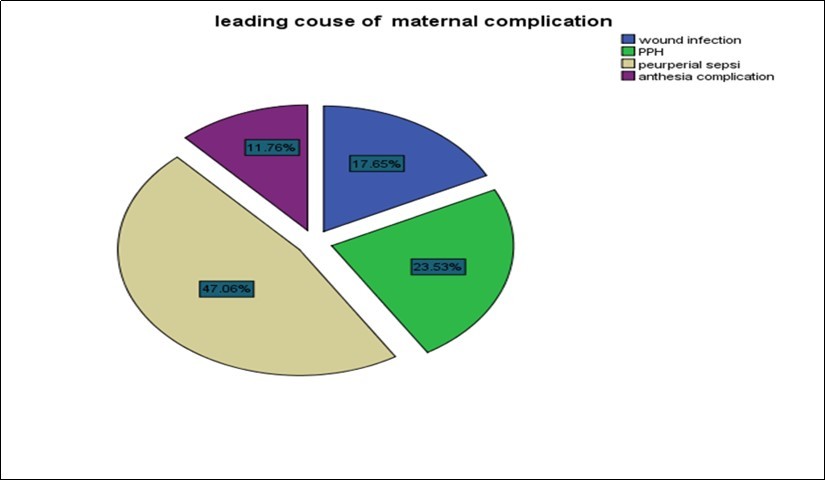
In this study, nearly all fetuses (82.7%) had a positive fetal heart beat at the time of admission, and majority (83.3%) of them presented with the vertex. Three-fourth of newborn babies (79.6%) had normal birth weight (2500-4000 gm). Higher than two-third of (79.6.4%) fetus had normal Apgar score (Table 2). Figure 3.
Table 2. Fetal Obstetrics related variables before and after CS intervention in Shenen Gibe General Hospital, south west Ethiopia, 2020| S.no | Fetal obstetrics variable | Frequency | Percent | |
| 1 | Fetal heart beat on admission | Positive | 154 | 82.8 |
| Absent | 32 | 17.2 | ||
| 2 | Fetal presentation | Cephalic | 155 | 83.3 |
| Breach | 28 | 15.1 | ||
| Others * | 3 | 1.6 | ||
| 3 | Fetal birth weight | <2500gm | 20 | 10.8 |
| 2500-4000gm | 148 | 79.6 | ||
| >4000gm | 18 | 9.7 | ||
| 4 | APGAR score | Zero | 11 | 5.9 |
| 3-6 | 27 | 14.5 | ||
| >7 | 148 | 79.6 | ||
Figure 3.Leading causes of perinatal deaths in Shenen Gibe General Hospital, south west Ethiopia, 2020
Among the total deliveries, 83(3.9%) newborns were stillbirths. The still birth rate among CS deliveries was 8.6%. There were 16 neonatal deaths following cesarean section. The four leading causes of neonatal mortality were perinatal asphyxia (45%), neonatal sepsis (22%), neonatal jaundice/MAS/HMD 8(19%), and meconium aspiration syndrome 6(14%).
Discussion
Cesarean section is the commonest obstetric operative procedure worldwide. When cesarean section is used appropriately it can improve the health outcomes of both the mothers and neonate. However, when used inappropriately the potential harm may exceed the potential benefit of cesarean section. World health organization recommends that the rate of CS should not exceed 15% in developing countries. The purpose of this study was to determine the cesarean section rate, maternal and fetal outcomes performed by integrated emergency surgical officer in shenen Gibe general Hospital.
In this study, the rate of cesarean section (CS) delivery was 11%. This finding was consistent with the WHO recommendation which is between 5-15% 17, 18. However, it was lower than studies conducted elsewhere in Ethiopia 12, 33, 34. In this study majority (63.6%) of cesarean section deliveries were conducted within the age ranged from 20-29 years, which is consistent with the study conducted in Sudan 8. This might be because of the reason that these age groups are the most reproductively active age group.
The finding of this study indicated that, the leading indication for cesarean section delivery was fetal distress; it accounted 25% of all the cesarean section which was consistent with the finding at southern Ethiopia, and Yekatit 12 hospital in Ethiopia 35 while, fetal distress proportion in this study was higher than studies at Jimma university specialized hospital 12, Nigeria and Pakistan 26. The higher proportion of fetal distress responsible for Cesarean section delivery might be due to the use of intermittent auscultation and nature of amniotic fluid as means of fetal monitoring during labor in the study center, because there were no facilities for electronic fetal monitoring in this study.
Although the cesarean section rate in this study was in line with the WHO recommended range, the two years of retrospective data analysis indicated that; two hundred six babies died in all forms of delivery and 42 neonates were died following cesarean section procedure, giving the overall neonatal mortality rate of 98.8% per 1000 live birth and a proportion of 16.8% neonatal death due to cesarean section delivery. Similar finding was reported in Ethiopia at Black lion hospital and Jimma Hospitals 11, 12.
On the other hand, in this study among the total 2267 total deliveries, eight mothers were died, giving the overall maternal mortality ratio 353 per 100,000 live births, while maternal mortality following cesarean section delivery accounted 12 per 1000 live births, which was higher than the finding from Jimma University specialized Hospital 12. Besides maternal deaths, 28% of the mothers develop one or more illness following cesarean section delivery, majority of the poor health outcomes other than death was noted among mother whose age between 40-49 years. The major causes of maternal illness was wound infection (46%), hemorrhage (PPH) (23%), anesthesia complication (17%) and sepsis (14%), which was higher compared with the finding from Jimma 36, 37. The higher proportion of poor health outcomes of the mother following cesarean section delivery was due to the poor pre-operative preparation (preoperative prophylaxis), cleanness of the surrounding environment, and poor follow-up.
As limitation, outcomes of cesarean section delivery that were discharge at home from the hospital were not assessed. In addition, the nature of the study which was retrospective data analysis misses some variables.
Conclusion
The cesarean section rate of 11.0% of observed in this review is within the recommended range by the WHO for developing countries (5%-15%). The health outcome of both the mother and neonate following cesarean section delivery was worrisome. Hemorrhagic shock and respiratory failure was the major causes of maternal deaths. While, cephlopelivic disproportion (including failure to progress secondary to arrest disorder) was a major maternal indication for poor maternal health outcomes. Therefore, timely and adequate progress of labor evaluation should be conducted. In addition, fetal heart rate monitoring in labor is recommended to reduce the suspected fetal distress. Moreover, basic maternal health service and basic emergency obstetric care should be strengthening. Furthermore, establish neonatology unit near to the maternity ward to prevent neonatal hypothermia is very essential.
References
- 2.Weil O, Fernandez H. (1999) Is safe motherhood an orphan initiative?The. , Lancet 354(9182), 940-943.
- 3.Landon M B, Hauth J C, Leveno K J, Spong C Y, Leindecker S et al. (2004) Maternal and perinatal outcomes associated with a trial of labor after prior cesarean delivery.New England. , Journal of Medicine 351(25), 2581-2589.
- 4.DeCherney A, Nathan L, Goodwin T M, Laufer N. (2012) Current diagnosis and treatment obstetrics and gynecology: McGraw-Hill Medical;.
- 5.Akasheh H, Amarin V. (2000) Caesarean sections at Queen Alia Military Hospital, Jordan: a six-year review.
- 7.Victora C G, EML Aquino, M do Carmo Leal, Monteiro C A, Barros F C.. Szwarcwald CL: Maternal and child health in Brazil: progress and challenges.The Lancet 377(9780), 1863-1876.
- 8.Betrán A P, Merialdi M, Lauer J A, Bing-Shun W, Thomas J et al. (2007) Rates of caesarean section: analysis of global, regional and national estimates.Paediatric and perinatalepidemiology. 21(2), 98-113.
- 10.Souza J P, Gülmezoglu A, Lumbiganon P, Laopaiboon M, Carroli G et al. (2010) Caesarean section without medical indications is associated with an increased risk of adverse shortterm maternal outcomes:. the 2004-2008 WHO Global Survey on Maternal and Perinatal Health.BMC medicine 8(1), 1.
- 11.Silver R M, Landon M B, Rouse D J, Leveno K J, Spong C Y et al. (2006) Maternal morbidity associated with multiple repeat cesarean deliveries.Obstetrics &. , Gynecology 107(6), 1226-1232.
- 12.F Ben Onankpa MBBS. (2009) Fetal outcome following cesarean section in a university teaching. , hospital.Journal of the National Medical Association 101(6), 578.
- 13.James R, Scott R S, Gibbs B Y, Karlan A F. (2003) Danforth's Obstetrics and Gynecology.Translated to Persianby: Ghadi Pasha A, Karimi MI Tehran: Baraye FardaPub:. 377-378.
- 14.Hawkins J L, Koonin L M, Palmer S K, Gibbs C P. (1997) Anesthesia-related deaths during obstetric delivery in the United States. , The Journalof the American Society of Anesthesiologists 86(2), 277-284.
- 15.Leone T, Padmadas S S, Matthews Z. (2008) Community factors affecting rising caesarean section rates in developing countries: an analysis of six countries.Social science & medicine. 67(8), 1236-1246.
- 16.Stanton C, Ronsmans C. (2008) Recommendations for routine reporting on indications for cesarean delivery in developing countries.Birth. 35(3), 204-211.
- 18.UNICEF F.Monitoring emergency obstetric care: a handbook.Geneva, Switzerland: World HealthOrganization2009.
- 19.AAA Omar, SHA Anza. (2012) Frequency Rate and Indications of Cesarean Sections at Prince Zaid Bin Al Hussein Hospital-Jordan.JRMS. 19(1), 82-86.
- 20.Francome C, Savage W. (1993) Caesarean section in Britain and the United States 12% or 24%: is either the right rate?Social. , Science & Medicine 37(10), 1199-1218.
- 21.Thomas J, Paranjothy S. (2001) National sentinel caesarean section audit report. Royal College of Obstetricians and Gynaecologists Clinical Effectiveness Support Unit.London:. RCOG Press,200(1): 43
- 22.Lauer J A, Betrán A P. (2007) Decision aids for women with a previous caesarean section.British MedicalJournal. 7607, 1281.
- 23.RSN Rehan. (2000) N: Prevalence and determinants of caesarean section in a teaching hospital of. , Pakistan.Journal of Obstetrics and Gynaecology 20(5), 479-483.
- 24.Donnay F. (2000) Maternal survival in developing countries: what has been done, what can be achieved in the next decade.International. , Journal of Gynecology &Obstetrics 70(1), 89-97.
- 25.Liu S, Liston R M, Joseph K, Heaman M, Sauve R et al. (2007) System MHSGotCPS: Maternal mortality and severe morbidity associated with lowrisk planned cesarean delivery versus planned vaginal delivery at term.Canadian medicalassociation journal. 176(4), 455-460.
- 26.Berhan Y, Abdela A. (2004) Association EPH: Emergency obstetric performance with emphasis on operative delivery outcomes Does it reflect on the quality of care?Ethiopian journal of health development. 18(2), 96-106.
- 27.Cai W-W, Marks J S, Chen C, Zhuang Y-X, Morris L et al. (1998) Increased cesarean section rates and emerging patterns of health insurance in Shanghai. , China.American Journal of Public Health 88(5), 777-780.
- 28.Taffel S M, Placek P J. (1987) Liss T: Trends in the United States cesarean section rate and reasons for the 1980-85 rise.American journal of public health. 77(8), 955-959.
- 29.Green J E, McLean F, Smith L P. (1982) Usher R: Has an increased cesarean section rate for term breech delivery reduced in incidence of birth asphyxia, trauma, and death?American journal of obstetricsand gynecology. , 142(6 Pt 1, 643-648.
- 30.CSA I.Ethiopia demographic and health survey 2011.Addis Ababa, Ethiopia and Calverton,Maryland, USA: Central Statistical Agency and ICFInternational2012.
- 31.Gibbons L, Belizán J M, Lauer J A, Betrán A P, Merialdi M et al. (2010) The global numbers and costs of additionally needed and unnecessary caesarean sections performed per year: overuse as a barrier to universal coverage.World health report. 30, 1-31.
- 32.Central Statistical (2010) Agency [Ethiopia] and ICF International: Ethiopia Demographic and Health Survey 2010. In.Addis Ababa. , Ethiopia and Calverton, Maryland, USA;
- 33.Dey N, Hatai S. (1992) A study of caesarean section cases with special reference to maternal and neonatal. , outcome.Journal of the Indian Medical Association 90(6), 149-151.
- 34.Moges A, Ademe B W, Akessa G M. (2015) . Prevalence and Outcome of Caesarean Section in Attat Hospital, Gurage Zone, SNNPR, Ethiopia.Archives ofMedicine .
- 35.Mekbib T, Teferi B. (1994) Caesarean section and foetal outcome at Yekatit 12 Hospital. , Addis Abeba, Ethiopia 32(3), 173-179.
Cited by (1)
- 1.Alemu Hiwotemariam, Yigzaw Zeamanuel Anteneh, Asrade Lakachew, Nega Bantayehu, Belachew Amare, 2023, Proportion and associated factors of maternal complications of cesarean sections among mothers who deliver at Bahir Dar City Public Specialized Hospitals, Bahir Dar, Ethiopia, BMC Women's Health, 23(1), 10.1186/s12905-023-02388-y