
Hodgkin's Lymphoma In Low-Income Countries: Experience Of Togo
Abstract
While highly curable in developed countries, Hodgkin's lymphoma (HL), remains a significant challenge for resource-limited ones. This study aimed to describe the profile of HL in Togo. This was a retrospective, descriptive study conducted at the Clinical Hematology Department of the Campus University Hospital Center in Lomé, Togo. It focused on patient records diagnosed with HL between January 1, 2006, and December 31, 2022. Various variables such as age, gender, histological type of HL, Ann Arbor stage, prognostic classification, therapeutic protocol used, and patient outcomes were examined. The annual incidence of HL was 1.5 with a mean age of 38.7 years (range 12-63). Lymph node enlargement was the primary clinical sign (100%). Histologically, classical HL was found in 21 patients (87.5%). Staging was conducted for 16 (66.7%) patients, among whom 11 (66.7%) were at an advanced stage, and 6 (37.5%) had an unfavorable prognosis. The ABVD protocol was used in 13 patients (54.2%), receiving between 1 and 6 cycles. One patient achieved complete remission (4.1%), three deceased (12.5%), and 17 (71%) were lost to follow-up. Hodgkin's lymphoma prognosis remains unfavorable with low remission rates in Togo. Improving the technical facilities will ensure better management of this lymphoma.
Author Contributions
Academic Editor: Rada M. Grubovic, Macedonia, the Former Yugoslav Republic of
Checked for plagiarism: Yes
Review by: Single-blind
Copyright © 2024 Essohana Padaro, et al
 This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Competing interests
The authors have declared that no competing interests exist.
Citation:
Introduction
First reported by Thomas Hodgkin from the Guy’s hospital in London in 1832, Hodgkin lymphoma are a family of unique lymphoma subtypes, in which the nature of the neoplastic cell was enigmatic for many years 1. It’sremains a distinct entity among lymphoproliferative neoplasms due to its biological characteristics 2. It is characterized by nodal infiltration within a reactive tissue by voluminous tumor cells called Reed-Sternberg (RS) cells, essential for diagnosis but not entirely specific. The nature of the Reed-Sternberg cell has long been debated, but it is now well-established that it’s a neoplasm derived from B cells, in which the unique cellular microenvironment plays an important role in accurate diagnosis and pathobiology. 3. The diagnosis of Hodgkin lymphoma in the modern era relies on an appropriate clinical setting, and morphological and immunophenotypic assessment 1. Clinical and biological data from the last thirty years have distinguished two major entities in HL: classical HL and nodular lymphocyte-predominant HL 4. It is a rare pathology but highly curable with well-defined recommendations based on various prognostic classifications and initial response to treatments, combining different chemotherapy protocol (ABVD, BEACOPP) and radiotherapy 5. In Togo, patients do not always have access to prognostic tools, which are crucial for treatment strategies. Hence, we conducted this study to describe the epidemiological, clinical, biological, and therapeutic aspects of patients diagnosed with HL, as well as their outcomes in a resource-limited country like Togo. Additionally, this study aimed to assess the evolution of management, five years after the last one 6.
Methods
This was a retrospective, descriptive study involving patient records diagnosed with HL between January 1, 2006, and December 31, 2022, spanning a 16-year period. The study was conducted at the Clinical Hematology Department of CHU Campus in Lomé, Togo. The diagnosis of HL was based on histology from lymph node biopsy and/or immunohistochemistry. Staging included chest, abdominal and pelvis computed tomography and bone marrow biopsy in advanced stages. The Lugano Ann Arbor classification 7 was used to assess staging. The prognostic classifications used were the European Organization for Research and Treatment of Cancer (EORTC) 8 for limited stages and the International Prognostic Score (IPS) 9 for advanced stages.
Results
In total, 24 records were included. HL accounted for 18.1% of lymphoid neoplasms (24/132) and 3.8% of malignant hematologic disorders (24/748) during the study period. The annual incidence was 1.5. The mean age of patients was 38.7 years (12-63), with a male predominance and a sex ratio of 1.7. Figure 1 describes the distribution of patients by age group.
Figure 1.Distribution of patients according to age groups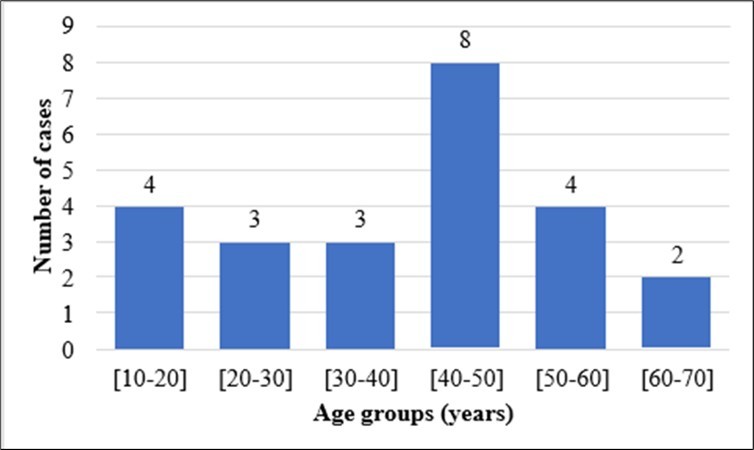
The main presenting circumstance of Hodgkin's lymphoma (HL) was lymph node enlargement, present in all patients (100%). Patients also exhibited night sweats (6/24), prolonged fever (6/24), fatigue (1/24), and persistent pruritus (1/24). Physical signs were predominantly characterized by lymph node enlargement, averaging 7cm (range 2-15). These were peripheral in 21 patients and cervical in 17. A quarter of the patients also presented with hepatomegaly, and four had splenomegaly.
Histologically, classical HL constituted most histological types, diagnosed in 21 (87.5%) patients. Table 1 illustrates the distribution of patients based on histology.
Table 1. Distribution of cases according to histological types| Numbers | Percentage | |
| Classical HL | 21 | 87,5 |
| Nodular sclerosis HL | 10 | 41,6 |
| Mixed cellularity classical HL | 6 | 25 |
| Lymphocyte-rich classical HL | 3 | 12,5 |
| Lymphocyte-depleted classical HL | 1 | 4,2 |
| Not specified | 1 | 4,2 |
| Nodular lymphocyte predominant HL | 3 | 12,5 |
Sixteen patients underwent staging (66.7%). Among these patients, five (33.3%) were at an early stage at diagnosis, with two patients presenting a bulky mass, and eleven (67.7%) were at an advanced stage (Figure 2). Adverse prognosis was observed in 37.5% of these patients (Table 2). Thirty-seven-point five percent (37.5%) of the included patients exhibited clinical signs of progression, and fifty-four percent (54%) showed biological signs of progression.
Figure 2.Distribution of patients according to Ann Arbor (Lugano) classification
| Numbers | Percentage | |
| EORTC Classification (Limited stage), n=5 | ||
| Favorable | 4 | 80 |
| Unfavorable | 1 | 20 |
| IPS Classification (Advanced stage), n=11 | ||
| Favorable | 3 | 27,3 |
| Unfavorable | 8 | 72,7 |
In terms of treatment, the frontline protocol used was the combination chemotherapy regimen of doxorubicin, bleomycin, vinblastine, and dacarbazine (ABVD). Thirteen patients, accounting for a ratio of 54.2%, initiated this treatment. They received between 1 and 6 cycles. Table 3 presents the outcomes of patients diagnosed with HL at the time of our study.
Table 3. Distribution of patients according to their outcome| Numbers | Percentage | |
| EORTC Classification (Limited stage), n=5 | ||
| Favorable | 4 | 80 |
| Unfavorable | 1 | 20 |
| IPS Classification (Advanced stage), n=11 | ||
| Favorable | 3 | 27,3 |
| Unfavorable | 8 | 72,7 |
Discussion
In comparison to other malignant hematologic disorders, Hodgkin's lymphoma is relatively rare, as demonstrated by the prevalence found in our study. With approximately 1,500 new cases per year in France, Hodgkin's lymphoma accounts for only 10 to 15% of lymphomas and 0.5 to 1% of new cancer cases 10. In the United States, it represents 10% of all lymphomas 11. In Togo, although the incidence of Hodgkin's lymphoma is low, it is on the rise. While it was 0.65 new cases per year in a study conducted over a 20-year period by Padaro et al. 6, it is currently at 1.5. This increase could be attributed to an improvement in technical facilities and an increase in the number of pathologists, making diagnosis more accessible. Hodgkin's lymphoma exhibits a bimodal distribution, with an initial peak in young adults (20-30 years) and a second peak in individuals over 60 years old 12. This bimodal incidence suggests that this pathology may stem from two distinct pathogenic processes: an infectious agent for young adults (EBV: Epstein Barr Virus) and a mechanism shared with other lymphomas for older patients 13, 14. In developing countries, Hodgkin's lymphoma predominantly affects a younger population. The average age of patients in our study aligns with this data, as do the findings of other sub-Saharan studies 15, 16. Hodgkin's lymphoma can also occur in children and adolescents, but it is rare before the age of 5 12. In our study, the low proportion of children found is explained by the fact that the hematology department at CHU Campus primarily receives adults. Male predominance has also been noted in previous series 11, 17, 18.
All patients presented with lymph node enlargement, predominantly peripheral and cervical. Indeed, at the time of diagnosis, most Hodgkin's lymphoma patients present with supradiaphragmatic lymphadenopathy. Patients frequently exhibit involvement of cervical, anterior mediastinal, supraclavicular, and axillary lymph nodes, while inguinal regions are less commonly affected. About a third of patients present systemic symptoms such as fever, night sweats, and weight loss 19.
Classical HL is the most found subtype, accounting for nearly 90% of HL cases 17, 18, 19. The results of our study align with this.
Only 16 patients (66.67%) underwent staging. This is mostly due to the patients' low socioeconomic status. Undergoing a scan cost approximately $133 USD, approximately 2.3 times the minimum wage during the study period ($58 USD). Long delays in specialized consultations, associated with diagnostic errors, and the difficulty in accessing the country's only public clinical hematology service account for the prevalence of advanced stages and poor prognoses in our study.
The indicated first-line treatment in our study was the ABVD protocol with six cycles, due to the unavailability of PET-CT at CHU and radiotherapy, which could have reduced the number of chemotherapy cycles based on the therapeutic response to systemic treatment. Only one patient achieved complete remission, and 17 (71%) were lost to follow-up. This high rate of loss to follow-up and low rate of remission reflects the financial precariousness of patients, most of whom did not initiate or complete the treatment. Indeed, Hodgkin's lymphoma is a highly curable hematologic malignancy, and the ABVD protocol is a validated treatment supported by several studies. It is used in combined therapy with radiotherapy or as a single modality due to the late toxicity of radiotherapy 20, 21, 22. The BEACOPP protocol is another effective therapeutic alternative for advanced stages. However, it is more toxic, requiring additional supportive care and closer monitoring of hematological parameters 23, 24, 25, making it unfeasible in our practice setting. Therefore, therapeutic strategy in Hodgkin's lymphoma relies on effective risk stratification based not only on the Ann Arbor classification but also on certain prognostic factors 7, 19. Beyond the historical classifications of EORTC for limited stages and IPS for advanced stages 8, 9, which have long guided therapeutic choices, PET-CT has proven useful both in diagnostic performance 26, 27, 28, 29 and in treatment 30, 31, leading to a modification in the therapeutic approach based on the response according to interim PET-CT after two cycles of chemotherapy. It is nowadays an indispensable tool for the effective management of Hodgkin's lymphoma.
Conclusion
Hodgkin's lymphoma is an infrequent lymphoma in our daily practice, even though its incidence is increasing. Its diagnosis is straightforward, relying on histology coupled with immunohistochemistry. Although the treatment is well-defined by various international recommendations, it poses similar challenges for practitioners in resource-limited countries, including prolonged diagnostic delays resulting in advanced disease and poor prognosis, inaccessibility to modern prognostic tools, and difficulty accessing standard or innovative therapies. All these factors lead to a low remission rate. Improvement in technical facilities and better social coverage will likely enable a more effective management of Hodgkin's lymphoma in Togo.
References
- 1.Wang H-W, Balakrishna J P, Pittaluga S, Jaffe E S. (2019) Diagnosis of Hodgkin lymphoma in the modern era. , Br 184-45.
- 3.Swerdlow S H, Campo E, Pileri S A, Harris N L, Stein H et al. (2016) revision of the World Health Organization classification of lymphoid neoplasms. , Blood 127(23), 75-90.
- 4.Alaggio R, Amador C, Anagnostopoulos I, Attygalle A D, O Araujo IB de et al. (2022) The 5th edition of the World Health Organization Classification of Haematolymphoid Tumours: Lymphoid Neoplasms. Leukemia.
- 5.Howlader N, Noone A M, Krapcho M, Garshell J, Miller D et al. (2023) . SEER cancer statistics review, 1975–2012. Natl Cancer Inst [Internet]. 2014; [cité 21 Disponible sur: https://hero.epa.gov/hero/index.cfm/reference/details/reference_id/3420543 .
- 6.Padaro E, Kueviakoe I, Magnang H, Layibo Y, Agbetiafa K et al. (2019) Cartéristiques épidémiologiques, clinico-biologiques, thérapeutiques et évolutives des patients atteints de la maladie de Hodgkin aux CHU de Lomé de 1999 à 2018. Burkina Méd. 23, 73-81.
- 7.Bd C, Ri F, Sf B, C F, Lh S et al. (2023) Recommendations for initial evaluation, staging, and response assessment of Hodgkin and non-Hodgkin lymphoma: the Lugano classification. , J Clin Oncol Off J Am Soc Clin Oncol [Internet]. 2014 [cité 21.
- 8.Diehl V, Stein H, Hummel M, Zollinger R, Connors J M. (2003) Hodgkin’s lymphoma: biology and treatment strategies for primary, refractory, and relapsed disease. Hematol Am Soc Hematol Educ Program. 22547.
- 9.Hasenclever D, Diehl V, Armitage J O, Assouline D, Björkholm M et al. (1998) A Prognostic Score for Advanced Hodgkin’s Disease. , N Engl 339(15), 06-14.
- 11.Miller K D, Nogueira L, Devasia T, Mariotto A B, Yabroff K R et al. (2022) Cancer treatment and survivorship statistics. , CA Cancer J Clin 2022, 40936.
- 12.Glaser S L, Jarrett R F. (1996) The epidemiology of Hodgkin’s disease. Baillieres Clin Haematol. 9-40.
- 13.Punnett A, Tsang R W, Hodgson D C. (2010) Hodgkin Lymphoma Across the Age Spectrum: Epidemiology, Therapy, and Late Effects. Semin Radiat Oncol. 20, 30-44.
- 14.Shenoy P, Maggioncalda A, Malik N, Flowers C R. (2011) Incidence Patterns and Outcomes for Hodgkin Lymphoma Patients in the United States. Adv Hematol [Internet]. Disponible sur: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3010617/ , cité 21.
- 15.Sawadogo D, Yapo A, Sangaré M, Tolo A, Yayo-Ayé M. (2009) Caractéristiques épidémiologiques des patients atteints d’hémopathies malignes à Abidjan au cours de la décennie 1995-2004. J Afr Cancer. 1, 4-10.
- 16.Ngolet L O, JDON Oval, Dokekias A E. (2018) Les hémopathies lymphoïdes chroniques à Brazzaville. Ann Sci Santé [Internet]. [cité 5 déc 2023] ;17. Disponible sur: https://www.annalesumng.org/index.php/ssa/article/view/261
- 17.Koffi K G, Sanogo I, Djigbenou D, Touré A H, Tolo A et al. (2000) Résultats du traitement de 62 cas de maladie de Hodgkin en Côte d’Ivoire. Bull Soc Pathol Exot. 93(5), 5-7.
- 18.Amégbor K, Darré T, Padaro E, Pegbessou E P, Bagny A et al. (2010) Profil histo épidémiologique des lymphomes au Togo: à propos de 755 cas observés au CHU Tokoin de Lomé. , J Afr CancerAfrican 2-23.
- 19.Ansell S M. (2022) Hodgkin lymphoma: 2023 update on diagnosis, risk-stratification, and management. , Am 97(14), 78-88.
- 20.Ng A K. (2014) Current survivorship recommendations for patients with Hodgkin lymphoma: focus on late effects. , Blood 124-33739.
- 21.Ng A K, MVP Bernardo, Weller E, Backstrand K, Silver B et al. (2002) Second malignancy after Hodgkin disease treated with radiation therapy with or without chemotherapy: long-term risks and risk. 100(19), 89-96.
- 22.Hodgson D C, van Leeuwen FE. (2015) Second Malignancy Risk After Treatment of Hodgkin Lymphoma. In : Engert A, Younes A, éditeurs. Hodgkin Lymphoma Compr Overv [Internet]. Cham :. Disponible sur : 375-409.
- 23.Bauer K, Skoetz N, Monsef I, Engert A, Brillant C. (2011) Comparison of chemotherapy including escalated BEACOPP versus chemotherapy including ABVD for patients with early unfavourable or advanced stage Hodgkin lymphoma. Cochrane Database Syst Rev [Internet]. Disponiblesur: https://www.cochranelibrary.com/cdsr/doi/10.1002/14651858.CD007941.pub2/full , cité 21.
- 24.André M, Bosly A. (2013) BEACOPPescalated versus ABVD in advanced Hodgkin’s lymphoma. Lancet Oncol. 14-9.
- 25.Wongso D, Fuchs M, Plütschow A, Klimm B, Sasse S et al. (2013) Treatment-Related Mortality in Patients With Advanced-Stage Hodgkin Lymphoma: An Analysis of the German Hodgkin Study Group. J Clin Oncol.
- 26.A C, H T, D A, S de G, G T et al. (2008) 18-F FDG-PET in the staging of lympho cyte-predominant Hodgkin’s disease. Haematologica [Internet]. [cité 21 nov 2023] ;93. Disponible sur: https://pubmed.ncbi.nlm.nih.gov/18166797/
- 27.C A, D R, Cr C, T L, C M et al. (2014) Initial staging of Hodgkin’s disease: role of contrast-enhanced 18F FDG PET/CT. Medicine (Baltimore) [Internet]. 93. Disponible sur: https://pubmed.ncbi.nlm.nih.gov/25121354/ , cité 21.
- 28.Jf G, V L, L T, M P, T C et al. (2014) Performance of FDG PET/CT at initial diagnosis in a rare lymphoma: nodular lymphocyte-predominant Hodgkin lymphoma. Eur J Nucl Med Mol Imaging [Internet]. , cité 21.
- 29.B-M E, P J, S A, M B, K W et al. (2015) Comparison of positron emission tomography/computed tomography with classical contrast-enhanced computed tomography in the initial staging of Hodgkin lymphoma. Leuk Lymphoma [Internet]. , cité 21.